Switzerland’s universal health system emphasizes individual responsibility, regulated competition, and decentralized governance. All residents are required to purchase basic health insurance from private nonprofit insurers (asylum seekers are automatically insured). Unlike many high-income countries, Switzerland’s basic health insurance premiums are standardized, determined by a person’s chosen insurer and their canton (region) not by their level of income. The government provides subsidies to low-income individuals and families.1
While the Federal Council (Bundesrat) determines the legal framework, setting out what is covered by OKP, the 26 cantons manage service delivery, hospital planning, and public health. This leads to regional flexibility but creates variation in access and efficiency.2
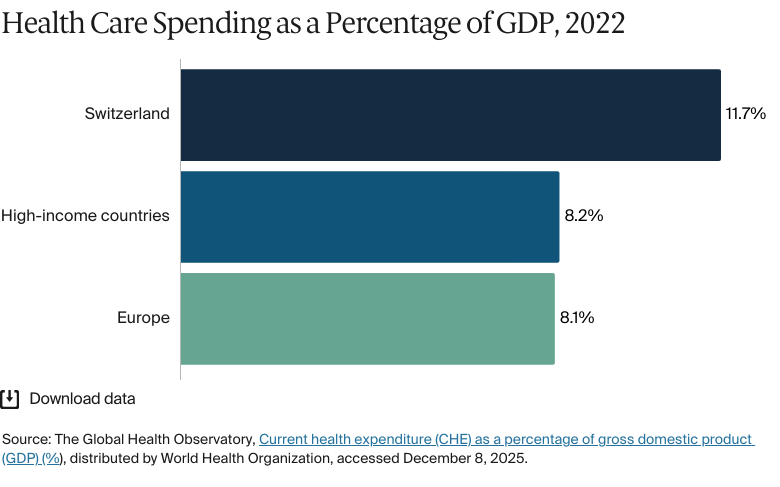
Health spending is among the highest in the world, at 11.7 percent of gross domestic product in 2022. Health outcomes are strong compared with those of other high-income countries, with high life expectancy and low infant and maternal mortality.3
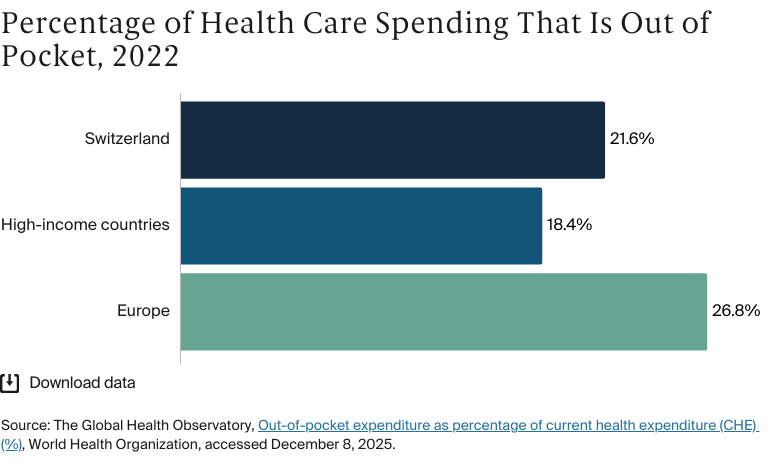
Patients pay a significant share of health care costs, including deductibles, coinsurance, and daily hospital fees, and out-of-pocket spending is higher than the European average.4 There is also growing pressure on the system from an aging population, workforce shortages, and fragmented care.5 Policymakers are now focusing on strengthening care coordination, expanding digital infrastructure, and containing costs.6
Universal health coverage is achieved through mandatory health insurance (obligatorische Krankenpflegeversicherung, or OKP), which all residents must purchase from private nonprofit insurers. Although offered by private entities, OKP is subject to stringent regulation, encompasses a standardized benefit package, and is publicly subsidized, effectively serving as the public insurance model.
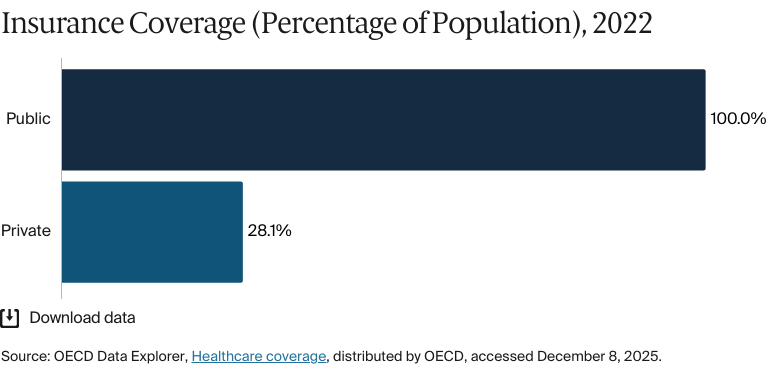
Public insurance coverage: 100% of population
Private insurance coverage: 28.1% of population
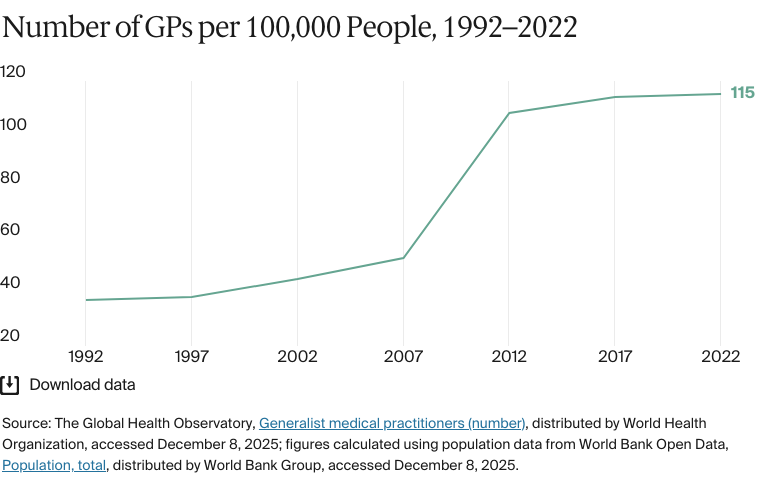
Primary care physicians: 115 per 100,000 people
Specialist physicians: 278 per 100,000 people
Switzerland spent 11.7 percent of its gross domestic product (GDP) on health care in 2022. Funding is drawn from a mix of sources. In 2023, 23 percent came from public funds, 45 percent from OKP, and 9 percent from voluntary private contributions.
Pharmaceutical spending: 11.5% of total health care budget
Out of pocket spending: 22% of total health care spend
Migrants in Switzerland are also less likely than Swiss-born residents to access health care. Barriers to access include language, high out-of-pocket costs (which are more likely to affect migrants, who earn less than Swiss-born residents, on average), and the lower likelihood that migrants will have a GP. Migrants are also more prone to experiencing mental health issues.
Income level and educational attainment is strongly associated with health outcomes. Disparities between urban and rural areas are also evident. Towns and cities have twice as many doctors as the countryside, and GPs in rural areas work longer hours.
The health system originated in the 19th century as sickness funds run locally by trade unions, churches, and cooperatives. Originally, these funds provided financial support to workers and their families if they needed help when ill; over time, they also began to offer reimbursements for treatment costs. By 1880, there were more than 1,000 funds, but these covered just 7.5 percent of the population.7 The share of the population with health insurance grew from about 11 percent in 1915 to 80 percent in 1959.8
The current coverage system was established by the 1994 Federal Health Insurance Act (Bundesgesetz über die Krankenversicherung, or KVG), which came into effect in 1996. The KVG introduced near-universal mandatory coverage, standardized benefits, community-rated premiums, and income-based subsidies, with insurers required to accept all applicants.9 Cantonal (regional) governments retained responsibility for planning acute and long-term care.10
Several revisions to the law since 2000 have focused on reducing high health expenditures.11 Nonetheless, Switzerland still spends more on health than the average for high-income countries.12
The Role of Public Health Insurance
Universal health coverage is achieved through mandatory health insurance (obligatorische Krankenpflegeversicherung, or OKP), which all residents must purchase from private nonprofit insurers. Although offered by private entities, OKP is subject to stringent regulation, encompasses a standardized benefit package, and is publicly subsidized, effectively serving as the public insurance model.13
The system is financed through premiums, direct payments by individuals, and contributions from both federal and cantonal governments.14 In 2023, 100 percent of the population was covered under OKP.15
All residents are required to purchase OKP within three months of birth or arrival in the country. This requirement applies to undocumented migrants (those who are unable to pay cannot access health care and must rely on support from nongovernmental organizations).16 All asylum seekers are covered by OKP, but cantons may limit the choice of insurers for such applicants.17
Federal authorities set the legal framework and approve premiums, while cantonal governments oversee hospital planning, provider licensing, and public health initiatives.
Services Covered by Public Health Insurance
Preventive care
Inpatient hospital care
Outpatient care
Maternity care
Primary care
Pharmaceuticals
Dental care
Eye care
Mental health care
Palliative care
Long-term care
Rehabilitation services
Home visits
Assistive devices.
All of these services are subject to cost sharing, which involves a minimum annual deductible (CHF 300 [USD 340]), 10 percent coinsurance (up to a cap), and a daily hospital fee.18 Some plans offer reduced premiums in exchange for higher deductibles or restricted provider choice.
Safety Nets
There are several protections to enable access for low-income and marginalized groups. Premium subsidies are available to residents with limited incomes and are financed jointly by the federal and cantonal governments.19 Each canton sets its own eligibility criteria and application process.
Children under age 18 are exempt from the annual deductible and daily hospital fee.20 Students age 25 and under who are in education or training programs are also exempt from the hospital fee. Women receiving maternity care don’t pay deductibles or coinsurance for prenatal, childbirth, or postnatal services.21 These exemptions reduce cost-related barriers for families, students, and expectant mothers.
The Role of Private Health Insurance
In addition to OKP, 28 percent of individuals in Switzerland purchase supplementary private insurance (Zusatzversicherung) on a voluntary basis.22 These plans cover services not included in OKP, such as dental care, alternative medicine, private or semi-private hospital rooms, and care received abroad.23
Unlike OKP, supplementary private insurance isn't regulated for universal access; insurers can reject applicants and vary premiums based on health status, age, and sex.24 Policies are purchased by individuals, but some employers offer partial contributions as a benefit.25
The Role of Government
Health care responsibilities are distributed across the federal, cantonal, and municipal levels of government. This decentralized approach enables national oversight while allowing services to be adapted to regional and local contexts.
The Federal Council regulates OKP under the KVG; defines minimum coverage standards; oversees pharmaceuticals, infectious disease control, and public health; and leads national policy through the Federal Office of Public Health (Bundesamt für Gesundheit, or BAG).26
Cantonal governments plan and fund hospitals, license providers, regulate working conditions for health personnel, and administer income-based premium subsidies.27
Municipalities support local health promotion (through infrastructure such as parks and sports facilities) and coordinate preventive initiatives.28
The government also works with private insurers, provider associations, and professional bodies such as the Swiss Medical Association (Foederatio Medicorum Helveticorum, or FMH), which is responsible for physician accreditation and continuing education. Citizens can influence national health policy through referendums.29
Integration and Care Coordination
Swiss health authorities have taken steps to promote more integrated and coordinated care, particularly for older adults and patients with complex needs. National strategies since 2017 have emphasized interprofessional collaboration, primary care strengthening, and better alignment between hospital and long-term care.30
Cantons play a significant role in the implementation of care. A national guide released in 2019 supports cantonal efforts to operationalize integrated care through local planning and feasibility tools.31 Building on this, the Health2030 (Gesundheit2030) strategy is designed to promote care coordination across settings by funding multidisciplinary teams, improving health data use, and supporting patient-centered service planning.32
Pilot programs, such as the Networks for Coordinated Care (Netzwerke zur koordinierten Versorgung), aim to improve outcomes and efficiency by offering bundled payments for services and coordination activities.33 Some of these models focus on integrated general practice, while others link acute and long-term care in rural regions.34 While there has been some progress, fragmented reimbursement systems and limited incentives for care coordination are persistent challenges.35
Efforts to coordinate care across settings are complicated by the decentralized governance structure. Each canton controls service delivery, leading to inconsistent adoption of integrated care models and health information technology infrastructure. This has contributed to the slow and uneven implementation of national initiatives, such as the electronic patient record36 (see Healthcare Technology).
Operations and Resources
Overview of the Delivery System
The health care system is organized into three main levels of care:
Primary care is delivered by general practitioners (GPs). This is the first point of contact for patients. It includes preventive services, chronic disease management, and treatment for common conditions.
Secondary care is provided by specialists and general hospitals, typically after referral. It covers diagnostics, specialist consultations, and more complex treatments.37
Tertiary care involves highly specialized services delivered at university hospitals and major referral centers. Such services include complex surgeries, intensive care, and rare or experimental treatments.38
Patients may access care at any level, depending on their insurance model. Basic OKP coverage includes direct access to specialists, but many Swiss opt for cheaper plans that require them to be referred by a primary care provider.39
Payment Mechanisms
Primary and outpatient care is reimbursed through a fee-for-service model governed by the national tariff schedule TARMED (to be replaced by the new TARDOC tariff schedule from January 202640), negotiated by insurers, provider associations, and federal authorities.41
Inpatient care is funded through SwissDRG, a fixed-rate case-based payment system introduced in 2012 that's jointly financed by insurers and cantonal governments.42
Long-term care is paid through care-dependent daily rates, with costs shared between OKP, patients (up to a cap), and public subsidies.43
Providersare paid either directly by insurers (known as third-party payer [tiers payant]) or by patients who are later reimbursed (third-party guarantor [tiers garant]), depending on contractual arrangements.44
Primary Care
Delivered by GPs, family doctors, and pediatricians, primary care is the foundation of the health system. These health care providers offer preventive services, chronic disease management, and treatment for common conditions.45 Residents are encouraged, though not required, to register with a GP to enable continuity of care and easier access to referrals.46
As of 2022, there were 115 primary care physicians for every 100,000 people.47 Urban areas, such as Zurich and Geneva, are better served than rural regions.48 Out-of-hours care is mandatory in some cantons; it is typically organized through GP cooperatives or on-call rotations.49
Outpatient/Specialist Care
Secondary care includes specialized outpatient and inpatient services delivered by hospitals, polyclinics, and medical specialists. It addresses conditions that go beyond the scope of primary care, such as complex chronic illnesses, specialized diagnostics, and surgical procedures.50
The basic OKP package includes direct access to specialists without having to be referred from primary care. However, about 70 percent of the population opt for cheaper options that require them to visit a primary care provider before being referred.51
As of 2023, there were 278 specialist medical practitioners for every 100,000 people,52 compared with an average of 262 across Organisation for Economic Co-operation and Development (OECD) countries in 2020.53
Over the past decade, there has been increasing consolidation into group practices and greater use of multidisciplinary clinics, particularly in urban centers.54
Physician Education and the Workforce
The physician workforce includes both public and private providers operating in a decentralized health system. An aging workforce — the average GP is 52 years old — has led to GP shortages, which have been exacerbated by restrictive policies on opening new practices.55 Advanced practice nurses (nurses with advanced diagnostic and prescribing responsibilities) increasingly support care coordination, especially in outpatient networks.56
Medical education, overseen by the Joint Commission of Swiss Medical Schools (Schweizerische Medizinische Interfakultätenkommission, or SMIFK), includes a state exam followed by three or more years of postgraduate training. Specialist certification requires six to seven years of practice in hospital departments related to the field of study.57 There are five accredited medical faculties (in Zurich, Geneva, Lausanne, Bern, and Basel).58 A federal initiative launched in 2016 has helped to increase the number of medical graduates from about 900 in 2016 to about 1,100 in 2021.59
For Swiss students, tuition is low; typically, it is CHF 500–1,000 (USD 567–1,135) per year. For international students, the annual tuition fees range from CHF 1,000 to CHF 4,000 (USD 1135–4540) per year.60
Switzerland is heavily dependent on international recruitment. As of 2021, 38.4 percent of doctors and 25.6 percent of nurses are foreign-trained.61 There’s little evidence of emigration by doctors trained in Switzerland.
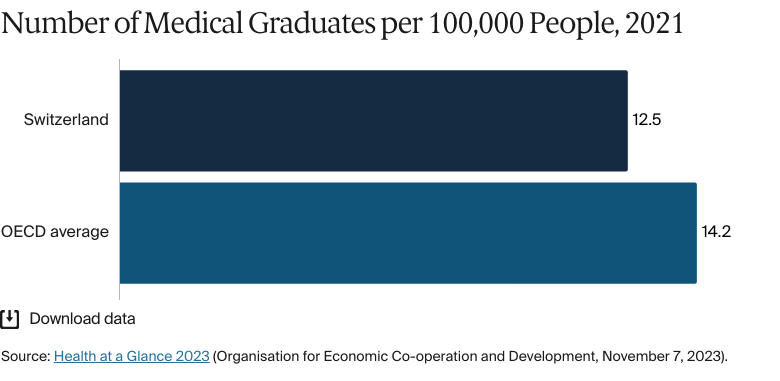
Despite expansion efforts, the country produced just 12.5 medical graduates for every 100,000 people in 2021 — below the OECD average of 14.2.62 Workforce sustainability will depend on improving domestic training capacity and incentivizing entry into primary care and rural practice.
Hospitals
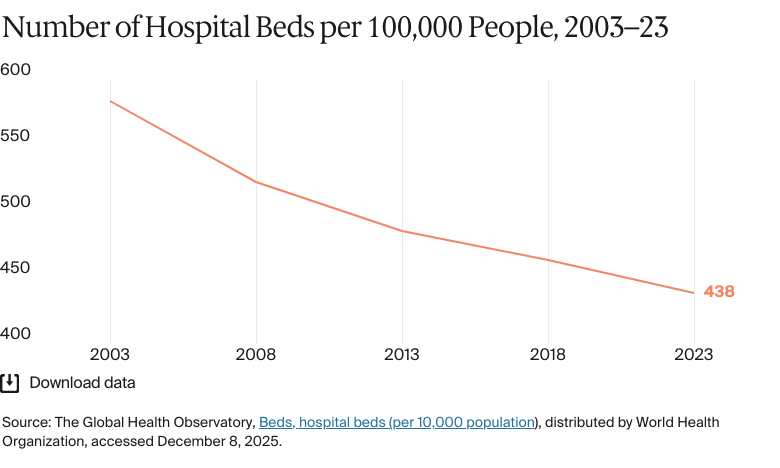
BY THE NUMBERS
In 2023, there were 438 hospital beds per 100,000 people63 (compared with 540 across high-income countries in 2020).64
In 2023, there were 1,919 nurses per 100,000 people65 (compared with 981 across high-income countries in 2021).66
Hospitals are publicly and privately owned. Public hospitals, run by cantons and municipalities, provide core inpatient care and are often affiliated with universities. Private hospitals, typically owned by nonprofit or corporate entities, focus on specialized or elective services.67
Hospitals operate under federal and cantonal regulation, including the KVG and the Hospital Planning and Financing Act (Spitalplanungs- und -finanzierungsgesetz, or SPFG).68 Cantonal authorities oversee licensing and integration into local service networks. Both public and private hospitals must meet national standards.69
Mental Health Care
BY THE NUMBERS
There were 53 psychiatrists per 100,000 people in 2023,70 significantly above the average of 13 for high-income countries in 2019.71
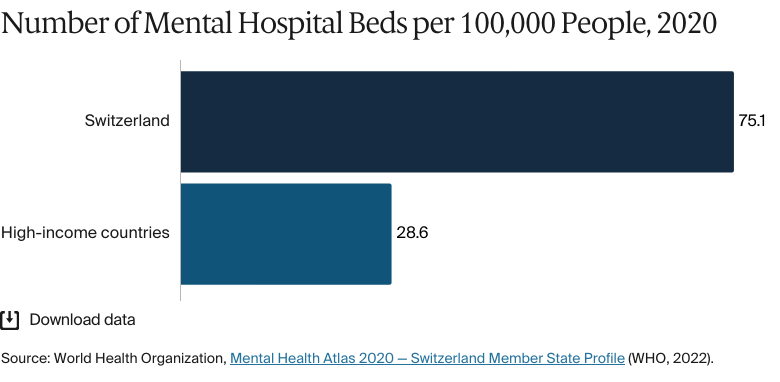
In 2020, there were 75 mental hospital beds per 100,000 people.72
Mental health services are covered under OKP and include psychiatric treatment, hospital care, and psychotherapy. Patients typically begin by consulting a GP, who can give them a referral for specialist care. Direct access to psychiatrists or psychologists is possible, but it is more likely to lead to higher out-of-pocket costs.73 Insurance covers 90 percent of approved treatment expenses, with patients responsible for coinsurance and deductibles.74
The high density of psychiatrists reflects a system that emphasizes specialist-led outpatient care, with many psychiatrists operating in private practice under OKP. In contrast, the number of mental hospital beds is relatively low (75 for every 100,000 people,75 compared with 29 for every 100,000 people across high-income countries in 202076), underscoring a shift toward community-based care and early intervention outside institutional settings. Access to psychotherapy often depends on a medical prescription or referral for sessions to be reimbursed by OKP, and the availability of therapists can vary considerably by canton, region, or language zone.77
Access has expanded over the last decade, with the inclusion of psychotherapy in OKP and the launch of public awareness tools, such as How Are You? (Wie geht’s dir?), which encourages talking about mental health, and Mental Health (SantéPsy), which offers practical advice and resources for the Latin cantons.78 Workplace mental health is supported through initiatives such as the Friendly Work Space label, which supports and encourages workplaces to promote their employees’ mental health.79
Long-Term Care and Social Support
Long-term care services include institutional care, home care, assisted living, and day and night care. National policy emphasizes home care before institutional care, and home-based services now support four times as many individuals as institutional care. The availability of long-term care services varies by canton.80
Long-term care is funded through both public and private sources. While public spending is comparable to that of other countries, including Germany, out-of-pocket costs are the highest among peer countries.81 Policymakers have proposed a mandatory long-term care insurance model to improve financial protection and expand coverage.
Workforce shortages are a growing challenge. Despite rising demand for home care, over 60 percent of the long-term care workforce is employed in institutional settings.82 Fifteen percent of the population over 50 was engaged in informal care in 2019, compared with the OECD average of 13 percent.83 Informal caregivers provide essential support but receive less financial assistance than in Germany or the U.K.84
Cost and Affordability
Health Care Spending Overview
Switzerland spent 11.7 percent of its gross domestic product (GDP) on health care in 2022 (the third highest globally), compared with an average of about 8 percent across high-income countries.85 In 2025, it spent USD 9,963 per capita on health, compared with the OECD average of USD 5,967.86
Funding is drawn from a mix of sources. In 2023, 23 percent came from public funds, 45 percent from OKP, 9 percent from voluntary private contributions, and 22 percent from out-of-pocket payments.87
An aging population, medical innovation, and rising demand are increasing costs.88 Efforts to manage spending have focused on expanding managed care, implementing activity-based hospital payments, and promoting digital health infrastructure.89
Pharmaceutical Spending
Pharmaceuticals accounted for 11.5 percent of total health care expenditure in 2021.90 In 2023, USD 1,061 per person was spent on medicines, making the country one of the three highest spenders in the OECD.91
There are several measures designed to promote the use of generic and biosimilar products. These measures include increased copayments for originator drugs, tiered pricing based on clinical benefit, and financial incentives for selecting lower-cost alternatives.92 To encourage the use of more affordable alternatives, copayments for original or reference drugs can reach 40 percent when a lower-cost generic or biosimilar is available. The reforms are projected to save CHF 250 million (USD 284 million) per year, although there are concerns about the impact on affordability for patients.93
A number of pharmaceutical reforms in 2024 have aimed to improve transparency or reduce costs. These include the use of a standardized benefit assessment tool for individual case reimbursement and changes to the pricing methodology intended to streamline administration.94
Cost Sharing and Out-of-Pocket Spending
Residents are responsible for out-of-pocket payments under OKP. These include an annual deductible, coinsurance (a retention fee), and a daily hospital charge.95
The standard deductible is CHF 300 (USD 340) per year. Higher deductibles can be selected in exchange for reduced premiums. Children under age 18 are exempt.96
A retention fee of 10 percent applies to costs above the deductible, capped at CHF 700 (USD 794) per year or CHF 350 (USD 397) for children.97
A hospital stay contribution of CHF 15 (USD 17) per day applies without a time limit, but there are exemptions for children, young adults in education, and maternity-related admissions.98
Some services are exempt from cost sharing, including maternity care, preventive services, and most general medical services during pregnancy and the postpartum period.99
Out-of-pocket spending accounted for 22 percent of current health expenditure in 2023, up from 21.7 percent in 2022. This compares with 18.4 percent on average in high-income countries and 26.8 percent across European countries in 2022.100 Annual cost-sharing caps apply to all services covered under basic insurance.101
How Are Costs Contained?
A series of national reforms has been launched to contain rising health care costs, led by the Federal Council’s cost containment program of 2018.102 The program promotes shared responsibility across the health system and is concerned with whether cost growth is medically justified.
Switzerland lacks transparency regarding health care quality. So we know that the Swiss health care system is costly, but we cannot assess whether this high cost translates into correspondingly high quality.
Rudolf Blanckart
Professor of Regulatory Affairs
KPM Center of Public Management, University of Bern and Swiss Institute for Translational and Entrepreneurial Medicine
Reforms have been rolled out in phases. Cost Containment Package 1a (Kostendämpfung — Paket 1a, or KP 1a), implemented in 2022 and 2023, introduced invoicing transparency, promoted outpatient flat-rate tariffs, and established a national tariff organization. In 2023, cost targets were introduced for OKP, offering a way to track cost trends based on demographics, price, and efficiency. Package 1b (KP 1b) took effect in 2024 and focused on enhancing cost monitoring by insurers, expanding pharmacists’ ability to dispense cheaper drugs, and simplifying rules for parallel imports.103
A second reform package was adopted in March 2025 (KP 2); this aims to expand the federal oversight of reimbursement and strengthen coordinated care.104
These measures build on earlier efforts under the Health2020 (Gesundheit2020) strategy, which achieved CHF 700 million (USD 768 million) in pharmaceutical savings. The Health2030 strategy continues this focus.105
Quality and Outcomes
BY THE NUMBERS
In 2021, average life expectancy was 83 years (compared with 80 in high-income countries).106
The top three causes of death in 2021 were:
Ischemic heart disease: 117 deaths per 100,000 people
COVID-19: 79 deaths per 100,000 people
Alzheimer’s disease and other dementias: 48 deaths per 100,000 people.107
The maternal mortality rate was 6 deaths per 100,000 live births in 2023 (compared with 11 on average in Europe).108
The infant mortality rate was 3 deaths per 1,000 live births in 2023 (the same as the average in the European Union).109
In 2021, the share of the population with mental health disorders was 18 percent (compared with 16% on average in high-income countries).110
The suicide rate was 12.7 deaths per 100,000 people in 2023 (compared with an average of 12 across high-income countries).111
There were two firearm-related deaths per 100,000 people in 2023.112
12 percent of adults were affected by obesity in 2022.113
Switzerland performs strongly on many health indicators compared with other high-income countries. Life expectancy is high, at 83.3 years, and rates of avoidable mortality, maternal deaths, and infant deaths are all below the OECD averages. Obesity prevalence is low, at 12.1 percent, and mortality from major noncommunicable diseases remains comparatively modest compared with the OECD average.114 However, mental illness affects 18.3 percent of the population, and the suicide rate is slightly above the average for high-income countries.
Addressing Health Inequities
People living in low-income districts have significantly shorter life expectancy, with the lives of men and women in disadvantaged areas up to 4.5 and 2.5 years, respectively, shorter than those of men and women in wealthier neighborhoods.115 Lower-income groups are also more likely to suffer from chronic illnesses. The implementation of premium reductions is down to individual cantons, meaning that levels of support vary significantly.116
Educational attainment is strongly associated with health outcomes: People without post-compulsory education report poorer health and face higher rates of preventable conditions, including lung cancer and musculoskeletal disorders.117 Meanwhile, healthy life expectancy gains have been concentrated among university-educated individuals. In 2014, they lived 8.8 years longer in good health than people with only compulsory education, with the gap having grown steadily in the years prior.118
Migrants in Switzerland are less likely than Swiss-born residents to access health care. Barriers to access include language, high out-of-pocket costs (which are more likely to affect migrants, who earn less than Swiss-born residents, on average), and the lower likelihood that migrants will have a GP.119 Migrants are also more prone to experiencing mental health issues.120
Disparities between urban and rural areas are also evident. Towns and cities have twice as many doctors as the countryside, and GPs in rural areas work longer hours.121 One tactic to address this is the expansion of telecare services, such as Remote Care Emmental, which uses digital technology to improve access to acute medical care in nursing homes.122
The Health2030 strategy identifies equity as a policy priority and outlines goals to improve affordability, expand digital access, and strengthen cross-sector collaboration.123
Innovation and Reform
Health Care Innovation
Several policy and structural reforms are aimed at improving care quality and encouraging innovation within the health system. A 2021 amendment to the KVG established a legal basis for quality improvement contracts between providers and insurers, coordinated by the Federal Quality Commission (Eidgenössischen Qualitätskommission, or EQK), which set out the metrics for quality delivery and sanctions for falling short of these.124 A renewed national strategy adopted in 2022 set four-year objectives for quality development, including requirements for performance measurement, reporting, and compliance, aiming to improve patient safety and the quality of health care.125
In 2024, voters approved a reform to align health financing more closely with outpatient care, which currently receives less public funding than inpatient services. The change is expected to save CHF 440 million (USD 499 million) annually by shifting more services to ambulatory settings.126
The Health2030 strategy outlines broad priorities for strengthening system responsiveness, including the better use of digital tools, improved care coordination, and more attention paid to long-term care needs.127 In 2024, the Switzerland Innovation Park East (Innovation Park Ost) launched a Health Innovation Hub to support partnerships in digital health, prevention, and medical technologies, with backing from research institutions and industry stakeholders.128
Health Care Technology
Switzerland has made gradual progress in digitizing its health system. Efforts have focused on improving coordination, patient safety, and access to care, with the centerpiece being the electronic patient record (EPR), introduced under the Federal Act on the EPR (Erarbeitung des Bundesgesetzes über das elektronische Patientendossier) and implemented in phases since 2022. Acute care hospitals, psychiatric clinics, and newly licensed medical practices are required to offer the EPR; participation by other providers and patients is voluntary.129 Adoption has been slow, however, held back by interoperability issues, decentralized governance, and resistance from both providers and patients.130
Digital transformation has been guided by the federal strategy eHealth Switzerland 2.0 2018–2024 (Strategie eHealth Schweiz 2.0 2018–2024), which has promoted the use of digital tools, citizen health literacy, and coordinated infrastructure.131 A long-term initiative launched in 2022, DigiSanté, sets out to standardize data exchange and build a legal and technical foundation for health data use through 2034.132 Telemedicine usage has also grown, particularly since the COVID-19 pandemic, and is improving access in rural areas.
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
De Pietro et al., Switzerland: Health System Review.↩
12
De Pietro et al., Switzerland: Health System Review.↩
13
“Healthcare Costs Rose to 91.5 Billion Swiss Francs in 2022” (Die Gesundheitskosten stiegen 2022 auf 91,5 Milliarden Franken) (Press Release, Federal Statistical Office [Bundesamt für Statistik], April 18, 2024), https://www.bfs.admin.ch/bfs/de/home/aktuell/neue-veroeffentlichungen.assetdetail.31225971.html; “In 2022, healthcare costs increased by 2.5% compared to the previous year. This increase is less pronounced than in the last five years (+3.2%)”.
↩
Generis Global Legal Services, “Healthcare system in Switzerland.
↩
30
Séverine Schusselé Filliettaz et al., “Integrated care in Switzerland: strengths and weaknesses of a federal system.” International Journal of Integrated Care 21, no. 4 (October 2021):10, https://doi.org/10.5334/ijic.5668.
↩
Tania Carron et al., “Integrated care models in Swiss primary care: an embedded multiple case study.” Journal of Evaluation in Clinical Practice 29, no. 6 (July 10, 2023):1025–38, https://doi.org/10.1111/jep.13891.
↩
Luca Steeman et al., “Out-of-hours primary care in 26 European countries: an overview of organizational models.” Family Practice 37, no. 6 (December 2020):744–50, https://doi.org/10.1093/fampra/cmaa064.
↩
D Elmer et al., “EPH58 changes in the number of different categories of specialists in Europe.” Value in Health 27, no. 6, suppl. (June 2024):S163–S164, https://doi.org/10.1016/j.jval.2024.03.887.
↩
54
“Swiss Primary Care Doctors Give Their Healthcare System Highest Marks in International Comparison” (Press Release, News Service Bund, February 14, 2023), https://www.news.admin.ch/en/nsb?id=93048.
↩
World Health Systems Facts, “Switzerland: medical training.”
↩
59
Stéphanie Giezendanner et al., “The ecology of medical care in Switzerland: prevalence of illness in the community and healthcare utilisation in Switzerland.” Swiss Medical Weekly 150, no. 1920 (2020):w20221, https://doi.org/10.4414/smw.2020.20221.
↩
João Mauricio Castaldelli-Maia et al., “WPA global survey on psychiatry in WPA member societies.” Asian Journal of Psychiatry 109 (July 2025):104559, https://doi.org/10.1016/j.ajp.2025.104559.
↩
World Health Organization, Mental Health Atlas 2020.↩
79
“Committed to systematic workplace health management” (Über uns Engagiert für systematisches BGM), Friendly Work Space, accessed December 8, 2025, https://friendlyworkspace.ch/de/engagiert-fuer-systematisches-bgm; “‘Friendly Work Space’ is an initiative of the Swiss Health Promotion Foundation. We are committed to the mental health of working people by supporting organizations in developing workplace health management systems.”
↩
80
Clara Lussi et al., “Trends over the past 15 years in long-term care in Switzerland: a comparison with Germany, Italy, Norway, and the United Kingdom.” BMC Geriatrics 24, no. 627 (July 2024), https://doi.org/10.1186/s12877-024-05195-8.
↩
“Pharmaceutical Measures: Measures to Promote Generics and Biosimilars” (Massnahmen Arzneimittel: Massnahmen zur Förderung von Generika und Biosimilars) (Press Release, Federal Department of Home Affairs [Eidgenössisches Departement des Innern] / Federal Office of Public Health [Bundesamt für Gesundheit], September 22, 2023), https://www.bag.admin.ch/dam/de/sd-web/Esppun5qaD-B/faktenblatt_generika_biosimilars.pdf; a press release reporting on changes to the rules for pricing generic and biosimilar medicines and increasing copayments for more expensive alternatives.
↩
“Health Insurance Act (KVG) amendment: cost containment measures — Package 2” (KVG-Änderung: Massnahmen zur Kostendämpfung — Paket 2), Federal Office of Public Health (Bundesamt für Gesundheit), March 21, 2025, https://www.bag.admin.ch/de/kvg-anderung-massnahmen-zur-kostendaempfung-paket-2; “the second cost-containment package ... [aims] to limit cost increases in mandatory health insurance to a medically justifiable level”.
↩
Institute for Health Metrics and Evaluation, GBD compare, distributed by IHME, accessed December 8, 2025, https://vizhub.healthdata.org/gbd-compare; overall firearm mortality is an aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
Organisation for Economic Co-operation and Development, Health at a Glance 2023.↩
115
André Moser et al., “What does your neighbourhood say about you? A study of life expectancy in 1.3 million Swiss neighbourhoods.” Journal of Epidemiology and Community Health 68 (April 2016):1125–32, https://jech.bmj.com/content/68/12/1125.
↩
“Social inequalities and physical health” (Soziale Ungleichheiten und körperliche Gesundheit), Federal Statistical Office (Bundesamt für Statistik), October 27, 2020, https://www.bfs.admin.ch/bfs/en.assetdetail.14817359.html; a survey assessing the percentage of the population meeting the health recommendations for physical activity.
↩
Christina Tzogiou et al., “What explains the inequalities in health care utilization between immigrants and non-migrants in Switzerland?.” BMC Public Health 21, no. 530 (March 2021), https://doi.org/10.1186/s12889-021-10393-9.
↩
120
Dawid Gondek and Laura Bernardi, “Mental health and wellbeing of population with migrant background in Switzerland: a scoping review and evidence map of quantitative evidence.” Journal of Immigrant and Minority Health 25, no. 5 (May 2023):1108–17, https://doi.org/10.1007/s10903-023-01490-5.
↩
eHealth Switzerland Strategy2018–2024 (Strategie eHealth Schweiz 2.0. 2018–2024) (eHealth Suisse, December 14, 2018), https://www.e-health-suisse.ch/payload/api/documents/file/Strategie_eHealth_Schweiz_2.0.pdf; “Goals and measures of the federal government and cantons for the dissemination of the electronic patient record and for the coordination of digitization surrounding the electronic patient record”.
↩
132
“Introduction” (Einleitung), DigiSanté, accessed December 8, 2025, https://www.digisante.admin.ch/de/programm; an overview of the purpose and implementation of the digital health strategy DigiSanté.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.