Roughly 55 percent of Medicaid enrollees are working full or part time, and a number aren’t eligible for health insurance through their jobs. Read more in an explainer here.
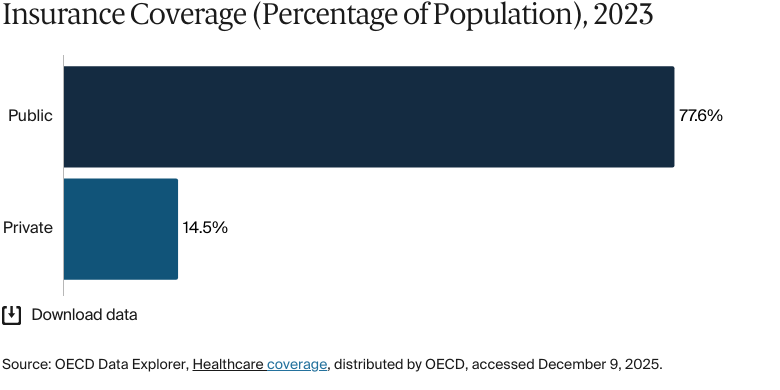
Mexico’s health care system is designed to provide universal coverage to all citizens and permanent residents, and the country has made significant progress toward this goal. As of 2023, public insurance covered 77.6 percent of the population, while 14.5 percent of the population had private insurance.1
Public health care in Mexico is funded primarily by federal and state contributions and by employer and employee payments.2 Care within the public system is delivered by a mixture of public and private providers, which are coordinated nationally by the Ministry of Health (Secretaría de Salubridad y Asistencia, later renamed the Secretaría de Salud).3
Major health system challenges persist. Per capita health spending is low compared with other countries in the Americas, and Mexico has the highest avoidable mortality rate among nations in the Organisation for Economic Co-operation and Development.4 There are critical public health challenges as well, from Indigenous health inequities to some of the world’s highest obesity rates. These challenges demonstrate the need to strengthen primary care and promote a healthier lifestyle.5
Mexico’s health care system has evolved through a century of reforms geared toward expanding access and strengthening the public health infrastructure. Its IMSS-Bienestar program is the main provider of free health care services for uninsured people.
Public insurance coverage: 77.6% of population
Private insurance coverage: 14.5% of population
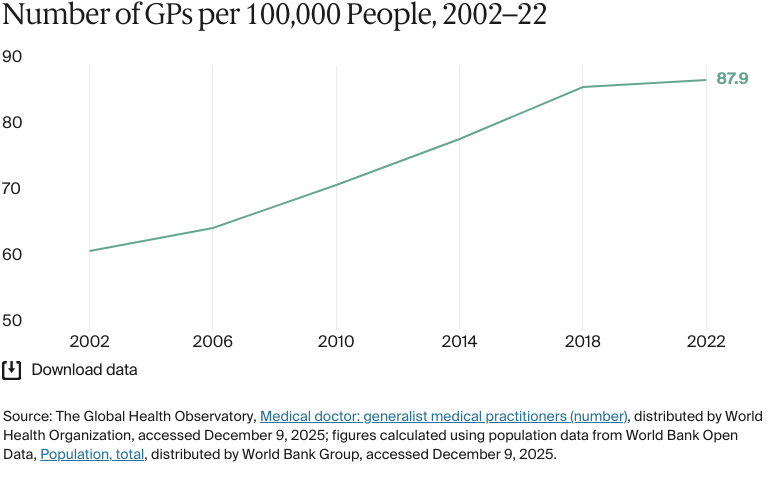
Primary care physicians: 87.9 per 100,000 people
Specialist physicians: 171 per 100,000 people
Total health care expenditure is increasing. In 2022, it reached USD 99 billion, up from USD 90 billion in 2017. Per capita spending has also continued to grow, reaching USD 66 in 2022, and is above the average for upper-middle-income countries (USD 585).
Pharmaceutical spending: 21% of total health care budget
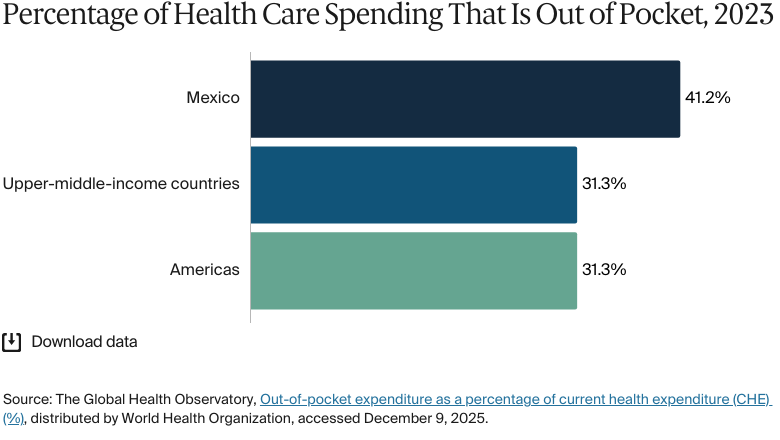
Out of pocket spending: 41.2% of total health care spend
There are stark disparities in health care access and quality, and progress in tackling health disparities has been uneven.
Rural and marginalized communities often struggle with limited medical facilities and insurance coverage, leading to poorer health outcomes compared with those in urban areas. Indigenous people, who make up 21 percent of Mexico’s population, experience higher rates of poverty, worse access to health care services, and an overall lower quality of care compared with that of other populations in the country. Women, especially those working informally as domestic workers, have historically lacked access to health care, labor protection, and social benefits.
Mexico’s health care system has evolved through a century of reforms geared toward expanding access and strengthening the public health infrastructure. The foundations were laid in the early 20th century, when employer-based insurance was introduced and public health efforts were launched to curb epidemics in urban and industrial areas.6 These efforts culminated in the establishment of legal rights to health and labor protection in the Constitution of 1917.7
In 1943, the government established the Mexican Social Security Institute (IMSS) for formal workers and the Ministry of Health (Secretaría de Salud) for uninsured people.8
This segmented system was expanded by the creation of the Institute for Social Security and Services for State Workers (ISSSTE) for government workers in 1959 and the National Program of Solidarity through Community Cooperation (IMSS-COPLAMAR) for rural communities in the 1970s. IMSS-COPLAMAR evolved into IMSS–Solidaridad in the 1980s and IMSS-Bienestar in the early 2020s.9
In the 2000s, the national health service, known as Seguro Popular, was introduced to reduce out-of-pocket costs and expand health care access for uninsured people.10 In 2020, it was replaced by the Institute of Health for Welfare (INSABI), which provided free, universal access to public health care. The system is noted for the affordability and quality of care it delivers, but structural fragmentation between the federal and state systems undermines its efficiency and accessibility.11
In 2023, INSABI was replaced by an expanded IMSS-Bienestar program. The Bienestar program then became the main provider of free health care services for uninsured people. Unlike its predecessor, IMSS-Bienestar operates independently of the federal ministries, and its greater autonomy allows it to coordinate its own improvement efforts.12 States must voluntarily transfer their health service responsibilities to the federal government to join IMSS-Bienestar. In 2022, 15 of 31 states had agreed to participate in the transition, covering 13 million people.13
The Role of Public Health Insurance
Access to the public health care system depends on employment status. This situation has resulted in a segmented system that is coordinated through multiple public institutions.14 The IMSS is a federal government health care institution that serves as the primary health care provider for anyone employed in the formal private sector, as well as for retirees and employees’ dependents. It accounts for over half of the country’s public health coverage and provides a wide range of services through its national network of hospitals and clinics.15
Public sector employees, such as teachers, police officers, and other government workers across federal, state, and municipal levels, are covered under the ISSSTE. In 2022, the ISSSTE insured more than 13 million people, including active employees, retirees, and their families.16 Similar employment-based structures exist for workers in state-owned enterprises, such as Mexican Petroleum, whose nearly 750,000 employees and dependents receive care through its own dedicated health care system. Members of the military are covered under the Social Security Institute for the Mexican Armed Forces.17
Services Covered by Public Health Insurance
The following services are covered by public health insurance:18
Preventive care
Primary care
Maternity care
Inpatient care (basic services are covered, but specialized surgeries or procedures may require out-of-pocket payments)
Outpatient care (certain diagnostic tests may incur out-of-pocket costs)
Pharmaceuticals (if they are listed on the national formulary of essential medicines)
Mental health care
Rehabilitative care.
Long-term care services are generally not covered under public health insurance (see Long-Term Care and Social Support). A few public institutions, such as the National Institute for Older Adults (INAPAM), offer limited long-term assistance to older adults without family or financial support, but these programs are small in scale (see Safety Nets). Similarly, pain management and hospice services for palliative care patients are not integrated into the public health care system.19
Safety Nets
Beyond the coverage for all citizens under IMSS-Bienestar, there aren’t many safety nets designed to promote equitable access to health care. IMSS-Prospera is a cash transfer program that targets low-income families (those living below the minimum well-being line) and provides financial assistance contingent on school attendance, routine health checkups, and nutritional support.20
Additionally, to support the aging population, INAPAM offers adults age 60 and over a discount card that reduces the prices of medications and medical consultations.21
The Role of Private Health Insurance
Public services are intended to meet the health needs of most of the population, but service shortages have created a growing reliance on private providers. For example, in outpatient care, two-thirds of hospitals and over half of outpatient clinics are privately operated.22 Uninsured individuals and lower-income groups that require private care because public services are unavailable often access this care through low-cost, pharmacy-based clinics.23
In 2022, 56 percent of Mexican adults needing health care sought it through private facilities — even though they were entitled to public services.24
The Role of Government
The government manages and oversees the health care system through a combination of centralized and decentralized mechanisms. At the federal level, the Ministry of Health is tasked with ensuring the population’s right to health protection as outlined in the Constitution. It supervises the implementation of policies and collaborates with state governments through agreements that define shared responsibilities. The ministry also regulates health services and oversees the coordination of the public and private sectors, although it does not have authority over the main social security institutions (the IMSS and ISSSTE).25
The IMSS is governed by an assembly and a technical council, both of which are made up of representatives from the federal government, trade unions, and employer organizations. The ISSSTE is governed by a similar board that includes representatives from various ministries and labor organizations.26
Coordination across different levels of government and health institutions is facilitated by the National Health Council and its state-level counterparts.27
Integration and Care Coordination
There has been a concerted effort to promote integration and care coordination across Mexico’s fragmented health care system. The 2016 National Agreement Toward the Universalization of Health Services, for instance, brought together state, federal, and social security institutions to coordinate efforts, standardize policies, and expand access to health services across the population.28
The government has also stepped up efforts to integrate care for the aging population within primary care. The pilot of the World Health Organization’s (WHO’s) integrated care for older people approach (ICOPE), for example, was implemented in Mexico City in 2020. ICOPE’s aim is to improve service delivery for older adults at the primary care level.29
Despite such initiatives, age-related care in Mexico continues to be underdeveloped and fragmented (see Long-Term Care and Social Support). Miguel Ángel González Block, of the Facultad de Ciencias de la Salud, Universidad Anáhuac, and director general at EviSys Consulting, “There is a serious lack of care coordination, especially in a country with rising levels of chronic conditions. If people rely on private care for primary services but then need hospitalization or specialty care and cannot afford it within the private sector, they go back to the public sector, repeating all the previous studies, delaying care. It is a very serious lack of coordination, with interruptions of care and so forth in a country where chronic diseases are ever more important.”
Operations and Resources
Overview of the Delivery System
The health care system operates across three levels of care:
Primary care is delivered through local clinics and health centers and serves as the first point of contact for patients. Treatment is focused on prevention, early detection, and basic care for common conditions.
Secondary care is typically delivered in general hospitals following a primary care referral for more complex diagnosis or treatment.
Tertiary care involves highly specialized treatments and procedures delivered in advanced specialty hospitals and national institutes.
Public health services are financed mainly through federal and state-level budgets or capitation payment mechanisms, which provide a fixed amount of funding per person regardless of the services used. Outpatient providers are paid through salaries, capitation, performance-based agreements, or fee-for-service arrangements. Public hospitals typically receive funding through budget allocations, but fee-for-service, diagnosis-related group, or per diem payments (which provide a fixed amount per inpatient day) can also be used for reimbursement.30
Primary Care
Primary care services are provided through public and private health care networks. The majority (76%) of primary care clinics are publicly owned and operated. There are a total of 6,735 registered private primary care facilities, with the vast majority (87%) operating as consulting rooms adjacent to pharmacies. These facilities offer lower-cost private care options for patients on low incomes.31
In 2025, Mexico had 231,000 general practitioners (GPs) and family practitioners. Of these, 189,000 were employed formally and 42,000 informally (meaning they worked without official employment contracts or job protections). In the same year, the average monthly salary for GPs and family practitioners was MXN 9,030 (USD 493).32
Emergency care services are available 24/7 at both public and private health care facilities. Staffed by GPs and specialists, they are accessible to everyone regardless of their insurance coverage (including the uninsured).33
Outpatient/Specialist Care
In the public sector, access to specialist care requires a referral from a primary care physician.34In 2022, there were 171 specialists for every 100,000 people.35
In the private sector, specialists operate mainly through self-referral systems. They are often located in consultation clinics adjacent to the country’s largest private hospitals, which are a source of referrals for high-tech diagnostics and hospital admissions. Private insurance covers most private hospital care, but insured patients are also reimbursed if they seek highly specialized treatment at Ministry of Health hospitals.36
Specialist physicians in Mexico are regulated by the National Normative Committee of Medical Specialty Councils under the Mexican National Academy of Medicine. More than one-fifth of the workforce is employed informally.37
Physician Education and the Workforce
Medical education typically lasts between six and seven years. Students must complete five years of medical school, followed by a one-year internship and an additional year of social service — often in underserved rural areas.38 There are public and private medical schools. Public institutions charge total tuition fees of up to MXN 12,000 (USD 655) for undergraduate programs, while private ones charge fees of up to about MXN 2 million (USD 109,111).39
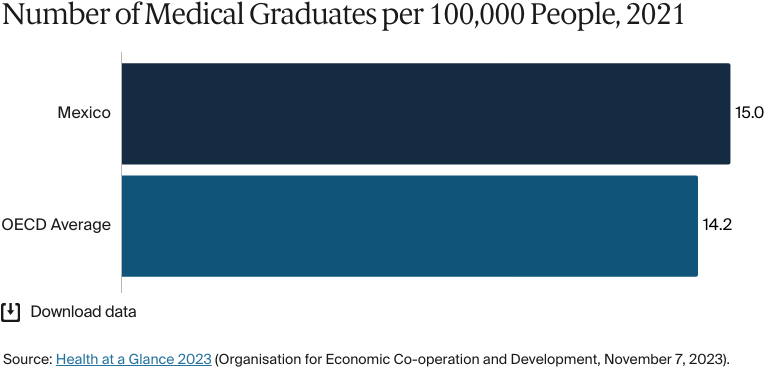
In 2024, there were more than 165 medical schools in operation, of which only 15 were accredited by the Mexican Council for the Accreditation of Medical Education.40 Even though roughly 17,500 physicians graduate and 12,500 specialists are licensed each year, the nation has a shortage of physicians.41 In 2023, there were 15 medical graduates for every 100,000 people.42
Rural areas are most affected by shortages, as physicians tend to prefer the higher compensation and better living conditions typically available in urban settings.43 To address this imbalance, the government has modestly raised salaries for physicians practicing in rural communities. It also invested nearly USD 24 million between 2022 and 2023 to recruit Cuban physicians to fill physician gaps. Although this initiative received criticism for its potentially exploitative labor practices, the government continues to support it as a solution to specialist shortages.44
Between 2018 and 2024, the government took a further step of increasing the number of medical residency training positions from 8,000 to more than 18,000, more than doubling the chance for doctors to specialize.45
Hospitals
BY THE NUMBERS
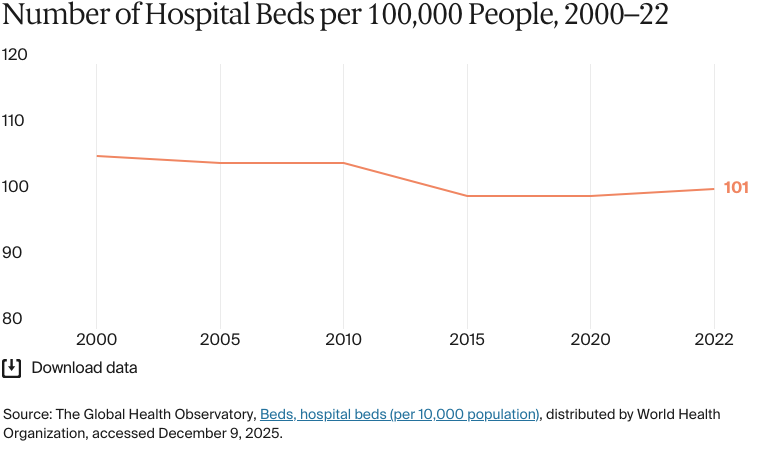
In 2022, there were 101 hospital beds per 100,000 people.46
In 2022, there were 303 nurses and midwives per 100,000 people (compared with 671 across the Americas).47
As of 2024, there are nearly 4,000 hospitals, of which 64 percent are private and 36 percent are public.48 Public institutions provide 70 to 80 percent of all health care services nationally. Between 25 and 30 percent of the population seeks care from private facilities, paid for through a mix of private insurance and out-of-pocket payments.49
The public hospital system is funded primarily through three federal agencies: the Coordinating Commission for National Institutes of Health and High-Specialty Hospitals, the Undersecretariat for Administration and Financing, and INSABI. These agencies finance infrastructure, personnel, and health care services across primary, secondary, and tertiary institutions.50
The private hospital sector has expanded steadily because of rising demand from higher-income individuals and international medical tourists, but overall bed capacity is limited compared with that in the public sector.51 Instead of employing permanent specialists, private hospitals generally rely on self-employed physicians who are granted clinical privileges by medical committees.52 Smaller private hospitals often operate as family-run businesses.53
Mental Health Care
BY THE NUMBERS
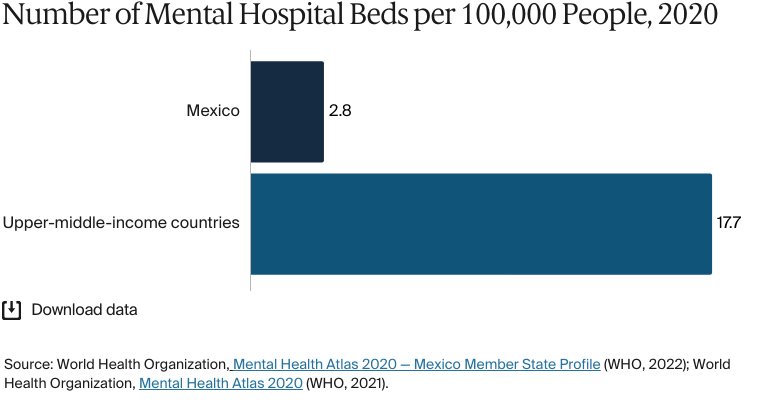
There were three mental hospital beds per 100,000 people in 2020 (compared with an average of 18 people in upper-middle-income countries).
There were 1.6 psychiatrists per 100,000 people in 2020 (compared with the 1.7 average for upper-middle-income countries).
There were 15 mental health professionals per 100,000 people in 2020 (the same as the average in upper-middle-income countries).54
Mental health care has undergone important reforms to move it from institutionalized care to community-based services. The 2013–2018 Action Program in Mental Health aimed to improve coverage and quality by integrating mental health care with primary health care.55 Since 2019, the government has implemented the WHO’s Mental Health Gap Action ;Programme to strengthen primary care services by training first-level health care personnel to identify and manage common conditions.56
Despite these efforts, access to mental health care remains uneven. In 2020, only 30 percent of primary health clinics offered mental health services, with most psychiatric services being concentrated in large urban centers: Over 40 percent of psychiatrists are based in Mexico City.57 As of 2021, there were only 39 psychiatric hospitals nationwide, 89 percent of which were located in major cities.58
Resource limitations also hamper the meaningful expansion of mental health care provision. In 2020, over 60 percent of spending was directed toward psychiatric hospitals rather than community services, and in 2021, just 2.2 percent of the total health budget was allocated to mental health.59
Long-Term Care and Social Support
Mexico lacks a formal long-term care system. No publicly funded services exist, and there are very few public residential institutions — only about 90 in 2020. Care for older adults and people with disabilities largely depends on unpaid family caregivers, who are primarily women.60
The number of older adults grew from 8.3 million in 2016 to 10.8 million in 2024 and is expected to rise in line with increasing life expectancy and declining birth rates.61
The government is taking steps to formalize care support. The National Institute of Geriatrics has developed competency standards for caregivers of seniors with functional dependencies. This step aligns with the broader National Care System, which aims to improve care quality and professionalize caregiving.62
In 2017, Mexico City enshrined the right to care in its constitution — recognition that all people are entitled to receive care that supports their well-being and enables them to live with dignity and participate in society throughout their lives. It also committed to creating a care system focused on serving people in situations of dependency, including situations related to illness, disability, childhood, or old age.63
In 2024, Jalisco became the first state to pass a law establishing an integrated public care system. This system guarantees the right to care, defines dependency, and assigns the responsibility for supporting both those who need care and those who provide it.64
Despite all this, the health care system for older adults remains fragmented across social security, government, and private insurance programs. In 2020, nearly 19 percent of older adults were unable to access the health care they needed.65
Cost and Affordability
Health Care Spending Overview
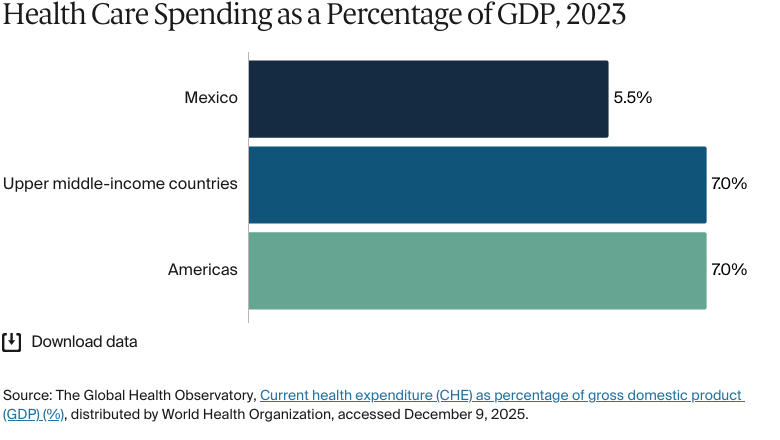
In 2023, health care spending accounted for 5.5 percent of gross domestic product (GDP), significantly lower than the average for upper-middle-income countries (7%) and the regional average for the Americas (7%).66
Total health care expenditure is increasing. In 2022, it reached USD 99 billion, up from USD 90 billion in 2017. Per capita spending has also continued to grow, reaching USD 766 in 2022, and is above the average for upper-middle-income countries (USD 585).67
In 2022, government spending accounted for USD 51 billion of total health care expenditure. The rest came from out-of-pocket spending (USD 39 billion) and prepaid private spending (USD 9 billion).68
In 2025, the federal budget allocated MXN 881 billion (USD 48 billion) to health services — a 12.2 percent cut from 2024 that aligned with the government’s goal to reduce public sector financial requirements from 5.7 percent of GDP to 3.9 percent by the end of 2025.69
Pharmaceutical Spending
Pharmaceuticals account for a significant portion of the total health care budget — 21 percent in 2022. In 2022, average per capita spending on medicines was about USD 292.70 In the private sector, most pharmaceutical expenses are paid out of pocket. Private insurers are gradually expanding drug coverage, but the market is still heavily dependent on direct payments by individuals.71
In the public sector, prices for patented drugs are negotiated by the Coordinating Commission for Negotiating the Price of Medicines and Other Health Inputs, with the aim of securing a single procurement price across public institutions.72
To control costs, the government promotes the use of generic drugs, which accounted for about 65 percent of market share in 2023. However, barriers limit market penetration for generics. An ongoing dependence on imports for active pharmaceutical ingredients, for example, leaves the country at risk of supply chain disruptions, and limited competition continues to slow the broader adoption of generics by hampering price reductions, availability, and awareness.73
In the private sector, price controls for patented products are based on a self-regulated maximum retail price system overseen by the Ministry of Economy (Secretaría de Economía).74 Maximum prices are set based on an international reference price that is adjusted by a market factor (an allowance that reflects the impact of conditions such as distribution costs and taxes).75 There is only limited enforcement of maximum prices, since participation is voluntary and there are no sanctions for noncompliance.76
Low-cost pharmaceuticals are a central reason for inbound medical tourism — especially from the U.S., where average drug prices are 172 percent of those in Mexico.77 However, prescription drugs are still unaffordable for most Mexicans, who face some of the highest costs after accounting for household income.78 A study examining the affordability of branded cancer medicines found that about 30 days’ worth of wages were needed to buy a day’s supply of a single treatment.79
Cost Sharing and Out-of-Pocket Spending
In 2023, out-of-pocket spending accounted for 41 percent of current health expenditure, significantly higher than the 31 percent average in the Americas.80
Anyone not enrolled in the IMSS through formal employment must pay a voluntary annual premium that is calculated according to age. As of 2024, the cost is:
MXN 8,200 (USD 447) for people ages 0 to 19
MXN 10,200 to 10,950 (USD 556 to 597) for people ages 20 to 39
MXN 12,700 to 13,150 (USD 693 to 717) for people ages 40 to 59
MXN 18,300 to 19,050 (USD 998 to 1039) for people ages 60 to 79
MXN 19,700 (USD 1075) for people age 80 and over.81
In 2020, 67.7 percent of households (24.2 million households) incurred out-of-pocket expenses. The largest proportions were for medications (39.9%), outpatient care (25.3%), and hospital care (20.3%).82
Between 2018 and 2020, the incidence of catastrophic health expenditure rose by about 18 percent. The rise mostly affected households with no health insurance.83 This continues to be a problem within the health care system, says Felicia Marie Knaul, distinguished professor of medicine, David Geffen School of Medicine, University of California, Los Angeles, and founding president, Tómatelo a Pecho, A.C.
Mexico has a huge issue with medical impoverishment and catastrophic health expenditure. Lack of access to care for chronic and noncommunicable diseases such as cancer and diabetes can be devastating for the poor — they can impoverish entire families.
Felicia Marie Knaul
Distinguished Professor of Medicine, University of California, Los Angeles
Founding President, Tómatelo a Pecho, A.C.
How Are Costs Contained?
To control rising health care costs while maintaining quality of care, outsourcing specialized medical services is becoming increasingly common. Dialysis treatment, for example, is now provided largely by private companies under contract with public health care agencies. Both public and private hospitals outsource surgical procedures to specialized firms or surgery centers.
This model allows hospitals to access advanced surgical techniques and equipment without the need for substantial capital investments in facilities or infrastructure. These services are provided on a pay-per-event basis and cover all necessary equipment, materials, pharmaceuticals, and surgical personnel.84 In addition, partnerships with U.S. health care providers have expanded access to specialized care, such as cardiac and cancer treatments.85
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
In 2025, average life expectancy was 75.7 years (compared with 74.2 years across upper-middle-income countries in 2021) — 72.6 years for men and 79 years for women.86
In 2021, the top three causes of death were:
COVID-19: 268 deaths per 100,000 people
Ischemic heart disease: 112 deaths per 100,000 people
The average maternal mortality rate was 42 deaths per 100,000 live births in 2023 (compared with 59 across the Americas).88
The avoidable mortality rate was 418 deaths per 100,000 people in 2022.89
The infant mortality rate was 11 deaths per 1,000 live births in 2023 (equal to the average across the Americas).90
In 2021, the share of the population with mental health disorders was 14 percent (equal to the average in upper-middle-income countries).91
The suicide rate was 7 deaths per 100,000 people in 2023 (equal to the average in upper-middle-income countries).92
The gun death rate was 21 deaths per 100,000 people in 2023.93
In 2022, 36 percent of adults were affected by obesity.94
Between 2019 and 2021, avoidable mortality from preventable and treatable causes increased significantly: from 393 deaths for every 100,000 people to 676. However, in 2022, the rate dropped to 418 deaths for every 100,000 people.95
In 2021, the leading cause of death in Mexico was noncommunicable diseases, which accounted for 53.6 percent of all deaths. This was followed by communicable, maternal, perinatal, and nutritional conditions at 38.8 percent. Injuries made up the remaining 7.6 percent.96
Overall patient satisfaction with health care is high in Mexico: For example, 87 percent of patients who have undergone inpatient surgery at public hospitals are satisfied with the service they received.97
Addressing Health Inequities
There are stark disparities in health care access and quality. Rural and marginalized communities often struggle with limited medical facilities and insurance coverage, leading to poorer health outcomes compared with those in urban areas. Public hospitals are frequently overcrowded and underresourced, and there are inconsistent standards of care across regions. Socioeconomic factors such as poverty and low levels of education further complicate health care access.98
Indigenous people, who make up 21percent of Mexico’s population, experience higher rates of poverty, worse access to health care services, and an overall lower quality of care compared with that of other populations in the country.99 Indigenous maternal mortality rates are twice as high, children experience a greater incidence of infectious diseases, and catastrophic health expenditures are more common.100 About half of Indigenous Mexicans live in rural, isolated communities that may lack health infrastructure, and many Indigenous people are distrustful of public health services, often relying on alternative medicine.101
Inequities also intensified during the COVID-19 pandemic, with the death rate in Indigenous communities being twice as high. Many communities rejected COVID-19 vaccines and surveillance to control disease spread because of their distrust of government health interventions.102
Gender-based inequities are also pronounced. Women, especially those working informally as domestic workers, have historically lacked access to health care, labor protection, and social benefits.103 The teenage pregnancy rate is one of the highest in the Organisation for Economic Co-operation and Development and is particularly high in Indigenous areas.104
Progress in tackling health disparities has been uneven. In 2004, Seguro Popular was introduced to extend universal health care coverage to marginalized populations. The 2020 dismantling of Seguro Popular and its replacement with INSABI ultimately reduced the coverage for many conditions, including chronic and severe illnesses, and placed between 40 and 60 percent of the financial burden on the patient. Women were particularly impacted, with INSABI doubling the number of uninsured women, leaving 16 million without access to affordable care.105
Innovation and Reform
Health Care Innovation
In 2023, 75 percent of adults and nearly 40 percent of children were overweight or obese, which has contributed to the increasing prevalence of chronic diseases such as diabetes and hypertension.106 To target the obesity crisis, since 2014, the government has:
Instituted a tax of one peso per liter on sugar-sweetened beverages
Introduced mandatory front-of-package nutrition warning labels to show sugar, fat, and sodium content
Enacted a ban on partially hydrogenated oils in line with global health recommendations
Prohibited the sale of ultra-processed foods in schools to promote better nutrition among students.107
Additional reforms to the health care system include the following.
2024–2030 National Health Plan
The 2024–2030 National Health Plan prioritizes disease prevention and expands 24/7 care by maximizing clinic and hospital capacity. It’s designed to strengthen the IMSS-Bienestar program by expanding access to universal free health care, increasing the availability and supply of medicines, and modernizing systems across all public facilities to make access easier.108
ISSSTE’s 2024–25 Strategy
ISSSTE’s 2024–25 strategy focuses on reintegrating privatized services such as cleaning and maintenance, stabilizing medication supply, and upgrading infrastructure. The plan also aligns with national health efforts, including joint vaccination drives with the IMSS and the Ministry of Health.109
Quality Improvement Initiatives
Mexico has introduced initiatives such as the HEARTS Quality Improvement Model. The HEARTS model is designed to enhance primary care services for cardiovascular disease prevention, particularly hypertension management. Promoted through national workshops, the initiative aligns local practices with global standards and aims to strengthen outcomes in primary health settings.110
Approaches to Chronic Diseases and Medicine Shortages
Other reforms introduced to improve Mexico’s health care include a nationwide chronic disease prevention campaign, the rollout of 31 hemodynamic units for advanced cardiac care, and the country’s largest medicine procurement plan. These initiatives aim to reduce the burden of diabetes, hypertension, and chronic kidney disease on patients while improving the availability of medicine through a new e-prescription tracking platform.111
Health Care Technology
The IMSS’s electronic medical record (EMR) system gives doctors from 1,576 national units access to patients’ clinical histories.112 It covers visits, diagnoses, lab results, and prescriptions dating back to 2017 and aims to minimize redundancies such as repeated tests and lost records.113
With more than 53.7 million medical records and 2 billion prescriptions logged, Mexico’s EMR database is the second largest in the world.114 The director general of the IMSS has stated that the system is designed to be interoperable, allowing medical records to move seamlessly across institutions such as the IMSS, the ISSSTE, and IMSS-Bienestar. Discussions about the integration of public and private systems onto a universal national platform are ongoing.115
Telemedicine is growing in underserved regions. In 2024, the U.S. Trade and Development Agency partnered with Vasanta Comunicaciones and California-based 19Labs to pilot 50 rural telemedicine clinics in Oaxaca and Tabasco, with the long-term goal of expanding to 1,000 rural communities.116 SaludConectaMX, developed by Cornell University in the U.S., is integrating clinical and social indicators to manage pediatric cancer care through cooperative mobile health systems.117
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Health at a Glance 2023 (Organisation for Economic Co-operation and Development, November 7, 2023), https://doi.org/10.1787/7a7afb35-en; Institute for Health Metrics and Evaluation, All-cause total health spending, spending per person, 2022, distributed by IHME, accessed December 10, 2025, http://ihmeuw.org/7c7q.
↩
González Block et al., Mexico Health System Review.↩
9
González Block et al., Mexico Health System Review; Institute for Social Security and Services for State Workers (Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado), “H. Board of Directors of the ISSSTE” (H. Junta Directiva del ISSSTE), Gob.mx, accessed December 18, 2025, https://www.gob.mx/issste/acciones-y-programas/h-junta-directiva-del-issste; an overview of the governing board of Mexico’s Institute for Social Security and Services for State Workers, including its legal basis, composition, and main functions; “History of IMSS Bienestar” (Historia del IMSS Bienestar), Gob.mx, accessed December 18, 2025, https://imssbienestar.gob.mx/04_historia.html; “IMSS Bienestar Health Services [is] ... the institution in charge of continuing the consolidation and execution of the strategy of centralizing health services to provide free medical care and medicines to people without social security”.
↩
10
González Block et al., Mexico Health System Review.↩
11
González Block et al., Mexico Health System Review; Gob.mx, “IMSS Bienestar.”
↩
12
Luis Javier Cortés-Adame and Octavio Gómez-Dantés, “The termination of Seguro Popular: impacts on the care of high-cost diseases in the uninsured population in Mexico.” The Lancet Regional Health — Americas, 46, no. 101078 (June 2025), https://doi.org/10.1016/j.lana.2025.101078; Mexican Social Security Institute (Instituto Mexicano del Seguro Social), “IMSS Bienestar evolves into a decentralized public body with greater capacities to strengthen the health system” (Evoluciona IMSS Bienestar a órgano público descentralizado con más capacidades para levantar sistema de salud), Gob.mx, August 30, 2022, https://www.gob.mx/imss/prensa/evoluciona-imss-bienestar-a-organo-publico-descentralizado-con-mas-capacidades-para-levantar-sistema-de-salud; an overview of how the reform into a Decentralized Public Body [Órgano Público Descentralizado] provides IMSS Bienestar with greater administrative and operational autonomy to expand and improve health services.
↩
“National Institute for Older Adults” (Instituto Nacional de las Personas Adultas Mayores), INAPAM, accessed December 16, 2025, https://inapam.com.mx/index.html; the home page of INAPAM, a government institution in Mexico dedicated to promoting the well-being, inclusion, and rights of people over 60 through social, educational, health, and recreational programs.
↩
22
Svetlana V Doubova et al., “Users’ perception of quality as a driver of private healthcare use in Mexico: insights from the People’s Voice Survey.” PloS One 19, no. 6 (June 25, 2024): e0306179, https://doi.org/10.1371/journal.pone.0306179.
↩
23
González Block et al., Mexico Health System Review.↩
González Block et al., Mexico Health System Review.↩
26
González Block et al., Mexico Health System Review.↩
27
González Block et al., Mexico Health System Review.↩
28
Committee on Economic, Social and Cultural Rights, List of Issues in Relation to the Combined 5th and 6th Periodic Reports of Mexico (United Nations Digital Library, 2017), https://digitallibrary.un.org/record/1317942?ln=en&v=pdf.
↩
29
Taking the Pulse of the Health System’s Response of the Needs of Older Persons: Situational Analysis Mexico (Pan American Health Organization, last updated December 22, 2022), https://iris.paho.org/handle/10665.2/56878.
↩
30
González Block et al., Mexico Health System Review.↩
31
González Block et al., Mexico Health System Review.↩
González Block et al., Mexico Health System Review; Ministry of Health (Secretaría de Salud), “Care for people without social security is guaranteed in public health centers: Insabi)” (Atención a personas sin seguridad social se garantiza en los centros públicos de salud: Insabi), Gob.mx, accessed July 30, 2025, https://www.gob.mx/salud/prensa/002-atencion-a-personas-sin-seguridad-social-se-garantiza-en-los-centros-publicos-de-salud-insabi?idiom=es; “The Institute of Health for Welfare (Insabi) reports that all people in the country who do not have social security have the right to receive free public health services, medicines and other associated supplies when they require care”.
↩
34
González Block et al., Mexico Health System Review.↩
“How much does it cost to study medicine? Is it cheap? 2025 guide” (¿Cuánto cuesta estudiar medicina? ¿Es barato? Guía 2025), Marco Estudiante en Linea, accessed December 18, 2025, https://marcoestudianteenlinea.com.mx/universidades/medicina/cuanto-cuesta; an overview of the typical costs of studying medicine in Mexico, showing the significant differences between public and private university tuition and overall expenses.
↩
40
Diego Ramonfaur and Octavio Gómez-Dantés, “Mexico’s physician shortage: struggling to bridge the gap.” The Lancet Regional Health — Americas 12, no. 41 (January 2025):100966, https://doi.org/10.1016/j.lana.2024.100966.
↩
41
Ramonfaur and Gómez-Dantés, “Mexico’s physician shortage.”
↩
Georgina Miguel-Esponda et al., “Implementation process and outcomes of a mental health programme integrated in primary care clinics in rural Mexico: a mixed-methods study.” International Journal of Mental Health Systems 14, no. 21 (March 16, 2020), https://doi.org/10.1186/s13033-020-00346-x.
↩
56
Miguel-Esponda et al., “Implementation process.”
↩
57
Miguel-Esponda et al., “Implementation process”; Immigration and Refugee Board of Canada, “Mexico: availability of health care and mental health services, including in Mérida, Mexico City, and Guadalajara; treatment of persons with mental illness by society and by the authorities; state protection, including recourse and complaints mechanisms available in cases of abuse (2019–July 2021),” European Country of Origin Information Network, September 9, 2022, http://ecoi.net/en/document/2080090.html.
↩
58
Martha Cordero Oropeza et al., “Community-based mental health services in Mexico.” Consortium Psychiatricum 2, no. 3 (November 5, 2021):53–62, https://doi.org/10.17816/CP86.
↩
59
Immigration and Refugee Board of Canada, “Mexico”; Cordero Oropeza et al., “Community-based mental health.”
↩
Government of Jalisco (Gobierno de Jalisco), “Law of the integral care system for the state of Jalisco” (Ley del Sistema Integral de Cuidados para el Estado de Jalisco), Periódico Oficial del Estado de Jalisco 42, s. 7 (2024), https://apiperiodico.jalisco.gob.mx/api/newspaper/getAsset?q=newspaper/21918/1708726570-2024-02-24-VII.pdf; official publication of the state law establishing the comprehensive care system for Jalisco; Zissis, “Mexico is growing old.”
↩
65
Sara Solis-López et al., “Age-friendly initiatives: Mexico.” Journal of Nutrition, Health and Aging 28, no. 1 (January 2024): 100007, https://doi.org/10.1016/j.jnha.2023.100007.
↩
66
The Global Health Observatory, Current health expenditure.↩
67
Institute for Health Metrics and Evaluation, All-cause total health spending 2022, distributed by IHME, accessed December 9, 2025, http://ihmeuw.org/7cb0; Institute for Health Metrics and Evaluation, Spending per person.
↩
68
Institute for Health Metrics and Evaluation, All-cause government health spending, 2022, distributed by IHME, accessed December 9, 2025, http://ihmeuw.org/7cb1; Institute for Health Metrics and Evaluation, All-cause out-of-pocket spending, 2022, distributed by IHME, accessed December 9, 2025, http://ihmeuw.org/7cb2.
↩
González Block et al., Mexico Health System Review.↩
73
Pharma Boardroom and OLIVARES, Pharma; Helly Kuveria et al., “Overview and lifecycle management of generic pharmaceutical drugs in Mexico, Guatemala and Brazil.” International Journal of Drug Regulatory Affairs 12, no. 2 (June 2024): https://doi.org/10.22270/ijdra.v12i2.676.
↩
Bram Sable-Smith, “American travelers seek cheaper prescription drugs in Mexico and beyond,” NPR, February 11, 2019, https://www.npr.org/sections/health-shots/2019/02/11/691467587/americans-seek-cheaper-meds-in-mexico; Andrew W Mulcahy et al., International Prescription Drug Price Comparisons: Estimates Using 2022 Data (RAND, February 1, 2025), https://www.rand.org/pubs/research_reports/RRA788-3.html.
↩
D Moye-Holz et al., “Availability, prices, and affordability of selected essential cancer medicines in a middle-income country: the case of Mexico.” BMC Health Services Research 20, no. 424 (May 14, 2020), https://doi.org/10.1186/s12913-020-05167-9.
↩
Roman Rodriguez Aguilar et al., “Out of pocket and catastrophic health spending in Mexico in the face of the COVID-19 pandemic.” EAI Endorsed Transactions on Pervasive Health and Technology 9 (May 9, 2023), https://doi.org/10.4108/eetpht.9.3583.
↩
83
Edson Serván-Mori et al., “Increase of catastrophic and impoverishing health expenditures in Mexico associated to policy changes and the COVID-19 pandemic.” Journal of Global Health 13 (October 27, 2023):06044, https://doi.org/10.7189/jogh.13.06044.
↩
84
International Trade Administration, “Mexico country commercial guide.”
↩
85
International Trade Administration, “Mexico country commercial guide.”
↩
86
National Population Council (Consejo Nacional de Población), Life expectancy at birth by federal entity according to sex, annual series from 2010 to 2025 (Esperanza de vida al nacimiento por entidad federativa según sexo, serie anual de 2010 a 2025), distributed by National Institute of Statistics and Geography (Instituto Nacional de Estadística y Geografía), accessed December 10, 2025, https://en.www.inegi.org.mx/app/tabulados/interactivos/?pxq=Mortalidad_Mortalidad_09_06a0d2ff-b4c8-44af-9e6d-420f4a59fbc2; “The average number of years a person is expected to live at birth, assuming that mortality trends remain constant, as this indicator is based on mortality rates for a given year”; The Global Health Observatory, Life expectancy at birth (years), distributed by World Health Organization, accessed December 10, 2025, https://www.who.int/data/gho/data/indicators/indicator-details/GHO/life-expectancy-at-birth-(years).
↩
Institute for Health Metrics and Evaluation, GBD compare, distributed by IHME, accessed December 9, 2025, https://vizhub.healthdata.org/gbd-compare/; overall firearm mortality is an aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
World Health Organization, Mexico: Health data overview for the United Mexican States, distributed by WHO, accessed December 9, 2025, https://data.who.int/countries/484.
↩
97
Svetlana V Doubova et al., “User experience and satisfaction with specialty consultations and surgical care in secondary and tertiary level hospitals in Mexico.” BMC Health Services Research 19 (November 21, 2019):872, https://doi.org/10.1186/s12913-019-4706-9.
↩
González Block et al., Mexico Health System Review; May Nguyen, “The disparity of indigenous and nonindigenous groups in the healthcare system of Mexico.” Global Insight: A Journal of Critical Human Science and Culture 1 (September 30, 2020), https://doi.org/10.32855/globalinsight.2020.002; Edson Serván-Mori et al., “Ethnic and racial discrimination in maternal health care in Mexico: a neglected challenge in the search for universal health coverage.” International Journal of Equity Health 24, no. 10 (January 12, 2025), https://doi.org/10.1186/s12939-024-02374-2.
↩
Cristina Espinosa da Silva et al., “Sexual and reproductive health awareness and practices among adolescents and adults in a rural farming community in Baja California, Mexico: a quantitative and qualitative cross-sectional study,” Sexual and Reproductive Health Matters 32, no. 1 (2024), https://doi.org/10.1080/26410397.2024.2433824.
↩
Juan A Rivera et al., “Perspective: Mexico’s experience in building a toolkit for obesity and noncommunicable diseases prevention.” Advances in Nutrition 15, no. 3 (March 2024):100180, https://doi.org/10.1016/j.advnut.2024.100180.
↩
“SaludConectaMX: lessons learned from deploying a cooperative mobile health system for pediatric cancer care in Mexico,” Cornell University, August 1, 2024, https://d10.48550/arXiv.2408.00881.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.