Background and History
In the 1940s, the newly independent Indonesian state inherited a fragmented and weak health system. It also faced the challenge of building a system that would cover the residents of the more than 17,000 islands that make up the country. Post-independence, the government focused on nationalizing private hospitals but struggled to adequately fund them. After President Suharto came to power in 1966, his New Order regime focused on development through market-oriented economic growth and introduced social insurance programs for civil servants, military personnel, and formal workers.
Community health centers (puskesmas) were introduced in 1968, improving access to health care, and by the 1970s, every subdistrict or area with a population of 30,000 to 50,000 had one. In 1979, smaller centers (pustu) were established at the village level — by 2013, these centers served populations of up to 3,000.
Although the government expanded public infrastructure — such as by building puskesmas — health care received limited operational funding. Public hospitals and health centers often lacked resources, and wealthier individuals turned to paid services at public hospitals. In 1986, the government legalized for-profit hospitals, further reinforcing the role of the private sector.
The 1997 financial crisis led to economic instability, prompting the government to launch the social safety net program (Jaring Pengaman Sosial Bidang Kesehatan), the first nationwide insurance for the poor. In 2004, the National Social Security Law (Sistem Jaminan Sosial Nasional) laid the foundation for universal health coverage through a greater focus on social welfare and equitable health care access.
In 2014, the government introduced its national health insurance program (Jaminan Kesehatan Nasional, or JKN), administered by the Social Security Agency on Health (Badan Penyelenggara Jaminan Sosial Kesehatan, or BPJS Kesehatan). JKN is intended to improve access to health care services and provide financial protection. BPJS Kesehatan manages contributions, claims, and provider networks.
The Role of Public Health Insurance
As of 2024, 97.6 percent of the population was covered under JKN. The program is available to citizens, permanent residents, and foreigners who have lived in the country for at least six months. JKN is funded through government budgets, employer and employee contributions based on salaries, and flat-rate premiums from informal and nonsalaried workers.
Under JKN, individuals employed in the formal sector are automatically registered by their employers. Although JKN is mandatory, integrating the informal sector, which employs a large proportion of Indonesia’s working-age population, remains difficult. Unlike formal sector employees and recipients of subsidized contributions, informal workers must voluntarily enroll in JKN, obtain membership cards, and pay their monthly contribution fees.
JKN previously divided inpatient care into three classes based on premium levels. These classes determined hospital ward amenities rather than the medical services provided. In 2024, the government began phasing in a new standardized inpatient class (KRIS) system and dismantling the previous system. The government aims to implement KRIS in nearly every hospital by summer 2025 to help all JKN patients receive the same quality of care.
Services Covered by Public Health Insurance
The following services are fully covered under public health insurance:
- Preventive care
- Inpatient care
- Outpatient care
- Maternity care
- Primary care
- Mental health care
- Palliative care
- Eye care
- Rehabilitative care.
Services that are partially covered:
- Dental care (advanced and cosmetic procedures are not covered)
- Long-term care (a public nursing program offers home care for the elderly through puskesmas, but this isn’t universally available).
JKN includes coverage with specific upper limits on value or quantity for certain medical devices:
- Eyeglasses are covered up to IDR 150,000 (USD 9) for third-class ward beneficiaries and IDR 300,000 (USD 18) for first-class ward beneficiaries for every two-year period.
- Hearing aids are covered up to a maximum of IDR 1 million (USD 60) for every five-year period.
- Medical assistive devices, such as wheelchairs and canes, are covered up to a maximum of IDR 2.5 million (USD 151) for every five-year period.
In accordance with Minister of Health Regulation No. 40/2012, the government prohibits copayments for services eligible under JKN and doesn’t impose an upper limit on treatment costs as long as they adhere to established clinical protocols. This regulation aims for all beneficiaries to receive necessary medical care at no additional cost beyond mandatory contributions to JKN.
Safety Nets
Some health care safety nets are designed to ensure access for all citizens. To improve accessibility to JKN, for instance, the government subsidizes premiums for people with low income.
The Family Hope Program (Program Kluarga Harapan) aims to improve child health and education outcomes and provides financial assistance to low-income families.
Beyond these government initiatives, many charitable clinics provide free medical services on a nonprofit basis. Some of these are supported by religious organizations. For example, a major Islamic non-governmental organization, the Muhammadiyah Society (Persyarikatan Muhammadiyah), currently has 125 hospitals across Indonesia.
The Role of Private Health Insurance
Private health insurance is uncommon in Indonesia, in part owing to the accessibility and affordability of JKN. Comprehensive private coverage demands high premiums, and there are multiple products with varying benefits. In 2021, only about 0.8 percent of Indonesia’s population used private health insurance.
Private health insurance is regulated by the Ministry of Finance (Kementerian Keuangan). BPJS Kesehatan has integrated programs from leading private insurers with public health insurance benefits, allowing middle- and high-income JKN members to access a top-up option. Private hospitals in Indonesia promise shorter wait times and better patient outcomes.
The Role of Government
The government organizes, plans, and regulates the health system, with responsibilities distributed among the central, provincial, and district governments.
At the central level, the Ministry of Health (Kementerian Kesehatan, or Kemenkes) is responsible for strategic planning, standard-setting, regulation, and resource allocation. It enacts laws and policies that guide the system but does not have authority over provincial or district health provision. Instead, it operates some programs that function at both the provincial and district levels, such as immunization programs.
At the provincial level, provincial health offices coordinate health services across districts and oversee provincial hospitals. They implement national policies within their jurisdictions and work to ensure the quality and accessibility of health care. Provincial health offices report directly to the provincial governor and align regional health services with national priorities while supporting district-level health care management.
At the district level, district health offices oversee district hospitals and manage the primary health services provided by puskesmas and their networks. District health offices implement health programs at the local level but don’t function under the authority of provincial health offices. Instead, they report to their district or municipal governments.
Multiple government agencies collaborate in the health sector beyond Kemenkes and BPJS Kesehatan. The Food and Drug Control Agency (Badan Pengawas Obat dan Makanan) regulates food and pharmaceutical safety, the National Population and Family Planning Board (Badan Kependudukan dan Keluarga Berencana Nasional) manages reproductive health initiatives, and the National Disaster Management Authority (Badan Nasional Penanggulangan Bencana) addresses emergency health care responses.
Integration and Care Coordination
Indonesia faces challenges in harmonizing its decentralized health administration and improving services. Strengthening regulatory enforcement, enhancing intergovernmental coordination, and expanding universal health coverage are all priorities for the government.
As of August 2024, 10,000 puskesmas had adopted the Integrated Primary Health Care (Integrasi Layanan Primer) program, which aims to unify fragmented health services at the primary care level. There is also a referral system that encourages patients to first seek care at puskesmas before being referred to hospitals.
Care is integrated through puskesmas and integrated health posts (posyandu). Puskesmas provide essential medical services, while posyandu, supported by volunteers, bring together a wide range of preventive care and health promotion activities, including mother and child health and nutrition (see Primary Care and Long-Term Care and Social Support).
Private primary care providers must collaborate with puskesmas on tasks such as communicable disease surveillance and government programs, such as immunization and family planning.
Overview of the Delivery System
Indonesia’s health care system has three tiers:
- Primary care focuses on essential health services, including preventive care and the treatment of minor illnesses and injuries. It is mainly provided through puskesmas and private clinics.
- Secondary care offers more specialized medical services, such as surgical procedures, obstetric care, and emergency treatment. These services are typically provided by district hospitals and private health care facilities.
- Tertiary care includes advanced and highly specialized treatments, such as organ transplants and cancer management. These services are typically available at referral hospitals and specialized private hospitals.
Primary health care providers are remunerated through a capitation system that covers outpatient services for 155 diagnoses, including diabetes, typhoid fever, and pneumonia. Treatment for some infectious diseases is instead covered by direct funding from Kemenkes.
Hospital reimbursements are determined by the Indonesian Case-Based Groups payment system, which groups similar diagnoses and procedures based on clinical and resource requirements.
Primary Care
The primary health care structure revolves around puskesmas, which provide vital services, such as vaccinations, health education, maternal and child health care, and chronic disease management. They are generally staffed by general practitioners (GPs), nurses, dentists, public health specialists, and midwives. However, in some rural areas, they are only staffed by nurses and midwives.
The health facilities that support puskesmas include pustu, which are mostly run by nurses and village health posts (poskesdes), which should have one nurse and one midwife. Posyandu are run by volunteers who promote health and focus on preventive care.
Each puskesmas is responsible for public health activities in its area and is supported by a diverse team of professionals. Some offer emergency services only during opening hours, but the ones with inpatient facilities provide 24/7 emergency care.
Primary care facilities are responsible for referring patients to secondary or tertiary care, ensuring that puskesmas focus on routine and preventive care to reduce burdens on hospitals.
Individual GPs, nurses, and midwives also run private primary health care clinics, often alongside their work in the public system. The World Bank estimates that there are about 9,000 private primary care clinics in Indonesia and 7,000 individual GPs operating privately.
A 2024 study revealed that 17.3 percent of JKN participants accessed primary care regularly (more than twice in a six-month period) and only 19.7 percent of fully subsidized members.
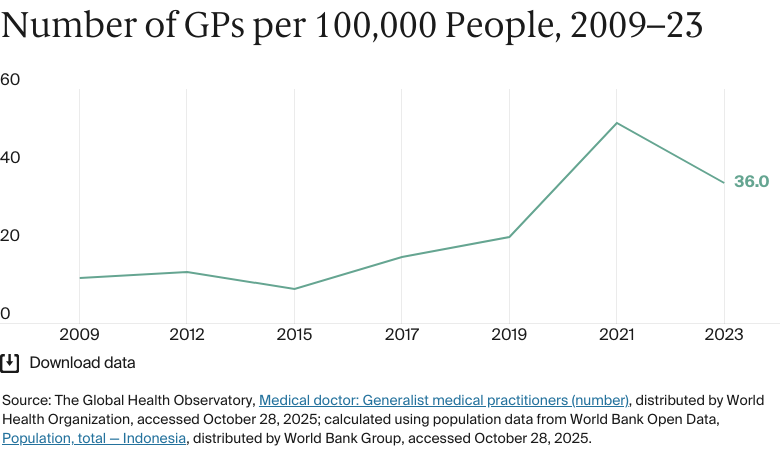
In 2023, there were 52.4 doctors for every 100,000 people, lower than the average across Southeast Asia in 2022 (77).
There are no data available for the proportion of doctors who are employed privately versus publicly.
Outpatient/Specialist Care
Typically, Indonesians access outpatient or specialist care by first obtaining a referral from a primary provider, such as a puskesmas or a general practitioner. Patients can use their JKN membership card at participating facilities. In emergencies, patients can skip the referral process and go directly to a hospital emergency department.
In 2023, there were 16 specialist medical practitioners for every 100,000 people.
Physician Education and the Workforce
In 2020, there were 88 medical schools, both public and private.
The undergraduate medical program requires at least 3.5 years of preclinical studies followed by two years of clinical training. Since 2010, graduates must complete a one-year internship after passing the national examination, then proceed to a two-year primary care physician program.
Annual tuition fees for medical school in Indonesia range from USD 3,000 to USD 6,100, on average. The University of Indonesia lists tuition fees of IDR 11 million (USD 656) to IDR 22 million (USD 1,313) per semester or IDR 44 million (USD 2,627) per semester for international students.
Specialist doctors are in short supply owing to the high costs of training and the relatively low pay. The distribution of medical workers is uneven: while Daerah Khusus Ibukota Jakarta has 0.6 doctors for every 1,000 people, East Nusa Tenggara has just 0.1 for every 1,000 people.
To address disparities and workforce challenges, the government has implemented a mandatory internship program after graduation that requires trainees to work in both rural and urban areas.
There are no data available for the percentage of doctors recruited from overseas or for those who choose to work overseas.
According to Diah Satyani Saminarsih, founder and CEO of the Center for Indonesia’s Strategic Development Initiatives, it’s crucial for volunteer community health workers to be formally integrated into the health workforce.
“Community health workers are not yet paid, so they’re seen as volunteers,” says Diah. “They haven’t reached the level of competency they should have because the district health [offices don’t] have the training material to make sure they can reach the level of proficiency required. We need to include them in the health workforce and stop seeing them as volunteers.”
Hospitals