Coverage and Access
Background and History
Iran’s health care system has evolved through significant reforms aimed at expanding access and improving equity. Modern medical education began in 1851 with the establishment of the Dār al-Fonūn school in Tehran. In 1910, legislation provided health care to specific groups, including military personnel and oil company employees, laying the groundwork for organized health services.
The establishment of the Ministry of Health in 1941 was the first step toward organizing the health care system on a national scale. In 1964, medical and other health‑related graduates were exempted from standard military service so they could participate in a mandatory public health service program.
Following the 1979 Islamic Revolution, Iran merged health care delivery with medical education in 1985 under the Ministry of Health and Medical Education (MoHME), which oversees hospitals, public health programs, and all medical universities nationwide. This combining of functions within a single ministry is relatively rare internationally. In that same year, the primary health care network was set up to provide community-based services through health houses (khaneh behdasht) staffed by trained community health workers (behvarz).
With the ultimate goal of universal health coverage, Iran launched the Health Transformation Plan (HTP) in 2014, which includes measures to expand insurance coverage, reduce out-of-pocket expenses, and improve the quality of hospital services.
The Role of Public Health Insurance
Four main organizations make up the public health insurance system, each covering a different segment of the population.
- The Social Security Organization (Sāzmān-e Ta'min-e Ejtemā'I, or SSO): The country’s largest public health insurer, the SSO covers over 50 percent of the population, serving private-sector employees, self-employed people, and some government-affiliated workers (such as employees of state-owned enterprises and quasi-government institutions, including national banks). Enrollment is mandatory for all formally employed and self-employed individuals. Contributions are 9 percent of the employee’s salary: 2 percent from the employee, 6 percent from the employer, and 1 percent from the government.
- The Iran Health Insurance Organization (Bimeh-ye Khadamāt-e Darmānī, or IHIO): The IHIO covers rural residents, civil servants, students, and informal-sector workers. Enrollment is automatic for rural residents, mandatory for civil servants, and voluntary for others. Refugees can also enroll in this program. Civil servants contribute 2.3 percent of their salaries, while coverage for rural residents and marginalized groups is funded by the government (though copayments apply for certain services at the point of access).
- Armed Forces Medical Services Insurance Organization (Sāzmān-e Bimeh Khadamāt-e Darmani-ye Nīrūhā-ye Mosallah, or AFMSIO): The AFMSIO covers active and retired military personnel and their families. Contributions are 7 percent of the employee’s wage: 2 percent from the employee, 2.5 percent from the employer, and 2.5 percent from the government.
Services Covered by Public Health Insurance
The public health insurance system offers a range of services through various benefit packages:
- Preventive care
- Primary health care (including mental health care, see Mental Health Care)
- Inpatient care
- Outpatient care
- Maternity care (preventive, childbirth, and prenatal care)
- Pharmaceuticals (prescription drugs in the Ministry of Health list)
- Emergency care
- Dental care (preventive)
- Rehabilitation services (partly covered).
Under most of the insurance plans, patients are responsible for 10 percent of inpatient service costs and 30 percent of outpatient service costs.
Members of the IHIO rural program benefit from reduced inpatient copayments of 3 percent when they use the referral system. Under this arrangement, 2 percent is covered by the MoHME, and 95 percent is funded by the IHIO.
Members of the SSO do not incur out-of-pocket expenses if they get services at SSO-owned facilities.
Safety Nets
The HTP was designed to reduce out-of-pocket expenditures and improve affordability, particularly for marginalized populations. It aims to do this by:
Expanding health insurance coverage. The HTP rapidly extended health insurance to about 10 million previously uninsured individuals, subsidizing or waiving premiums for low-income and/or rural populations. This expansion was facilitated by the IHIO.
Reducing copayment rates. The HTP introduced copayment caps to ease the financial burden for all individuals who require inpatient services in MoHME-affiliated hospitals. Copayments were set at a maximum of 10 percent for urban residents and 5 percent for rural residents. The HTP reduced these to 6 percent and 3 percent, respectively.
Introducing free health care for younger children. Iran’s primary care network has long offered free maternal care and child services, including immunization and routine well-child visits. In early 2024, authorities extended this by waiving charges for outpatient and inpatient treatment for children under age 7 in public facilities, with basic insurers covering the full public tariff.
The Role of Private Health Insurance
As the public health insurance system does not cover all medical expenses, about 20 percent of the population obtains private insurance to fill coverage gaps. This includes coverage for copayments, coinsurance, and services excluded from basic plans, such as certain dental and optical services.
The private health care sector plays a major role in the delivery of care, providing about 80 percent of outpatient services and 30 percent of inpatient services — some of which are funded by public insurance under service agreements with the MoHME. The private sector encompasses a range of providers, including independent practitioners, clinics, hospitals, diagnostic units, and pharmacies, which are licensed and regulated by the MoHME and its affiliated agencies, such as universities of medical sciences, at the provincial/local level.
Principal revenue sources are out-of-pocket payments and reimbursements from supplementary insurance. Patients pay directly for about 35 percent of the cost of private health services. The cost of services can also be high, further limiting lower-income households’ access to private health care.
Fragmented regulation and oversight are also challenges, leading to inconsistencies in service quality and pricing. In addition, the lack of integrated data systems has hampered effective monitoring and coordination between the public and private sectors.
The Role of Government
The government plays a central role in the health care system, primarily through the MoHME. Public-private partnerships (PPPs) create a hybrid model of direct service provision and regulated collaboration.
MoHME Responsibilities
Policy and regulation. The MoHME sets health policies and supervises the implementation of national health laws and regulations. It also develops clinical and public health protocols and licensing standards for health care facilities.
Health care delivery. Through universities of medical sciences, the MoHME owns and operates the majority of Iran’s public hospitals, including nearly all rural khaneh behdasht and urban comprehensive health centers. It also employs most of Iran’s health workforce.
Medical education and research. The MoHME oversees all medical universities, linking student training directly with public service delivery.
Pharmaceutical oversight. The MoHME regulates the production, import, distribution, and pricing of pharmaceuticals in coordination with the Iranian Food and Drug Administration (Sāzmān-e Ghazā va Dāru, or IFDA). This includes setting maximum retail prices and managing national drug procurement lists.
Integration and Care Coordination
One achievement in service integration is the incorporation of mental health services into primary health care. Launched in 1988, this MoHME initiative involved training general practitioners (GPs) and frontline health workers to provide basic mental health interventions at the community level.
Iran’s primary health care network also integrates basic oral health (including dental care units and school programs) and nutrition services (surveillance, counseling, and supplementation), which are delivered at khaneh behdasht and comprehensive health centers.
To address the needs of Iran’s aging population, the government launched the Integrated and Comprehensive Geriatric Care Program (Barnameh-ye Morāqebat-hā-ye Edqām-yāfteh o Jāme'-e Sālmandi) in 2017. Implemented across all primary health care centers, the program assembles multidisciplinary teams to offer personalized services tailored to older adults, including frailty screening and chronic disease management.
Other initiatives to improve integration include the promotion of PPPs to increase infrastructure and service quality. These collaborations have been implemented in areas including diagnostic services, hospital construction, and urban primary health care.
However, PPP initiatives face several challenges, including financial instability, a lack of clear legal frameworks, and coordination between public and private actors.
Operations and Resources
Overview of the Delivery System
The health care system has three levels:
Primary care is delivered at rural khaneh behdasht, urban health posts, and comprehensive health centers, which are staffed by behvarz and GPs. Many centers also employ dentists, nutritionists, psychologists, and occupational health experts. These facilities provide immunizations, maternal and child health care, chronic disease management, and other services.
Secondary care includes specialized services offered at district health centers and general/specialized hospitals, which serve as referral points for primary care facilities.
Tertiary care includes advanced diagnostics and treatment services that are delivered at specialist hospitals, many of which also function as training centers for health care professionals.
There are five principal payment methods for health care providers: salaries, capitation, fee-for-service payments, case-based payments, and performance-based payments.
At the primary care level, family physicians are typically paid monthly salaries funded by the MoHME. Primary health care clinics often operate under a capitation model (a fixed payment per patient).
In office and clinic settings, a fee-for-service model is most common, although providers may also receive a salary component, depending on the ownership and financing structure.
At the secondary and tertiary levels, provider payments are made through line-item budget transfers from the Plan and Budget Organization (Sāzmān-e Barnāmeh va Budjeh-ye Keshvar) to the provincial medical universities, primarily covering staffing costs.
Health insurance organizations, such as the SSO and the IHIO, purchase services using case-based payments for a basket of 90 high-prevalence procedures and fee-for-service payments for other procedures. Additionally, per diem payments compensate for hospital hoteling services (the provision of nonmedical amenities, such as meals, bedding, and room maintenance).
The SSO pays providers within its own facilities via global budgets and purchases services from external providers on a fee-for-service basis.
Despite these structured mechanisms, delayed payments from insurance funds create financial strain on health care facilities. Informal, under-the-table payments between patients and providers are widespread and undermine transparency and trust in the system.
Primary Care
The primary health care system is structured around a tiered referral network designed to promote universal access, preventive care, and early disease detection. Oversight is provided by the MoHME, which coordinates a multilevel infrastructure spanning rural and urban areas.
Health houses: In rural areas, the first point of contact is the khaneh behdasht, each serving between 1,000 and 1,500 residents.
Health posts and urban health centers: In urban areas, first-line care is delivered at health posts and urban comprehensive health centers. Health posts serve catchment areas of about 12,500 people and are staffed by “health protectors” (moraghebe salāmat), typically nurses or midwives with more formal clinical training than behvarz. Nutrition and mental health experts, dentists, and other professionals also work in the centers. Collectively, their responsibilities include chronic disease screening, health counseling, and managing noncommunicable diseases in urban communities.
Comprehensive health centers: Both rural and urban comprehensive health centers function as supervisory and referral hubs. They offer more advanced services — including diagnostics, dental care, and mental health interventions — and oversee the performance of frontline workers in their catchment areas.
One innovation in the primary health care system is the Each Home a Health Post initiative, launched in 2019 to enhance health literacy. During the COVID-19 pandemic, it helped strengthen the community response by mobilizing volunteers to support triage, contact tracing, and basic preventive care.
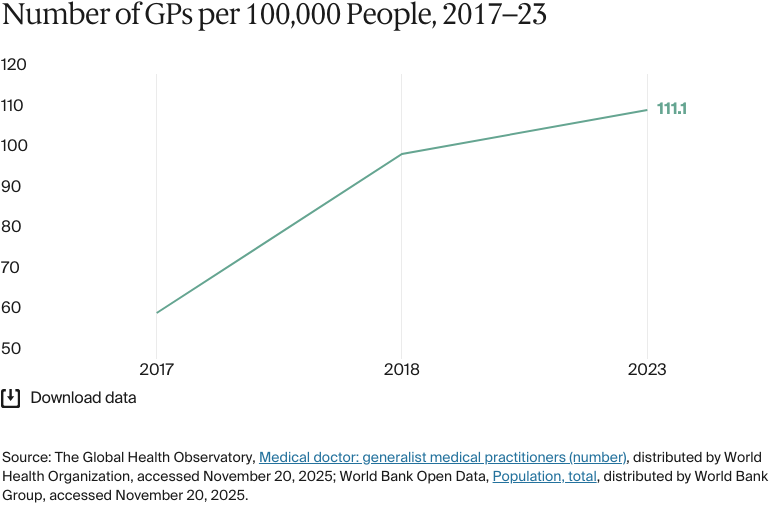
The primary health care system faces persistent workforce and financing challenges. In 2023, Iran had about 111 registered GPs for every 100,000 people, which is higher than in Turkey (73 for every 100,000 people) in 2022. However, in 2023 about 30,000 qualified GPs (about one-third of the workforce) were unwilling to practice, citing low pay and poor working conditions. In 2024, GP consultation fees per visit were set at IRR 1.26 million (USD 30), a rate that has not kept pace with inflation.
In addition, the distribution of primary care providers is inconsistent. More affluent cities, such as Tehran and Yazd, attract the majority of new graduates, while underserved rural regions, such as Sistan and Baluchestan, face persistent shortages. This inequity has prompted calls for stronger workforce incentives, targeted capitation reform, and better support for primary health care staff in remote regions.
Outpatient/Specialist Care
Secondary and tertiary health care services are delivered through a network of general and specialized hospitals as well as outpatient clinics. While the MoHME oversees the primary health care system, secondary and tertiary services are predominantly financed through public health insurance programs. The private sector also plays a significant role, especially in urban settings.
Despite an established hospital network, there are regional disparities in the distribution of specialist physicians. As of 2024, there were about 62 specialist doctors for every 100,000 people — significantly lower than the regional average of 143 and averages in developed nations, which range from 300 to 500 specialists for every 100,000 people. Over 52 percent of specialists are concentrated in just four provinces (Tehran, Isfahan, Khorasan Razavi, and Fars), which together account for only about 37 percent of the population.
In contrast, underserved areas, such as Sistan and Baluchestan, face critical shortages. In these regions, low specialist consultation fees contribute to disparities. As of 2024, specialist consultation fees were set at IRR 1.9 million (about USD 45) per visit. These fees are considered low, especially when compared with inflation and the cost of living, and have influenced where specialists choose to practice.
Physician Education and the Workforce
The medical education system is overseen by the MoHME, which integrates health care delivery and academic training. As of 2024, there were more than 60 MoHME-affiliated medical universities, which are responsible for educating and training 77 percent of the health workforce. Medical education is free for Iranian citizens studying at public universities.
The medical curriculum typically spans seven years: five years of theoretical and technical instruction followed by two years of clinical internship. Reforms have focused on competency-based education, interactive teaching, and alignment with global best practices.
Structured training pathways also exist for behvarz, who serve rural areas. They undergo a two-year preservice residential training program focusing on both theoretical and hands-on practical education under the supervision of district health networks.
Despite a strong educational infrastructure, a significant share of medical professionals, particularly physicians, nurses, and medical faculty, are emigrating in search of better opportunities. In 2022, 54 percent of doctors and nurses wanted to emigrate, citing economic instability, corruption, and poor governance. In 2022 and 2023, about 6,500 doctors (including 2,300 specialists) left the country — 30 percent higher than the number of incoming doctors. Interest in specialization declined: only 100 applicants applied for 385 residency positions, and some critical specialties, such as anesthesiology, had no applicants.
The health care system is also struggling with the uneven geographic distribution of professionals. Over 96 percent of medical graduates practice in urban areas, drawn by better pay, opportunities for professional advancement, and infrastructure, leaving rural regions underserved. Nurses are in short supply due to poor working conditions, low salaries (often less than USD 200 a month), and early retirement.
To address the nurse shortage, the government has attempted to expand the number of nursing schools and increase student intake. However, the mass departure of experienced faculty — 850 left their academic posts in the year ending March 2024 — further undermines the training pipeline.
Hospitals
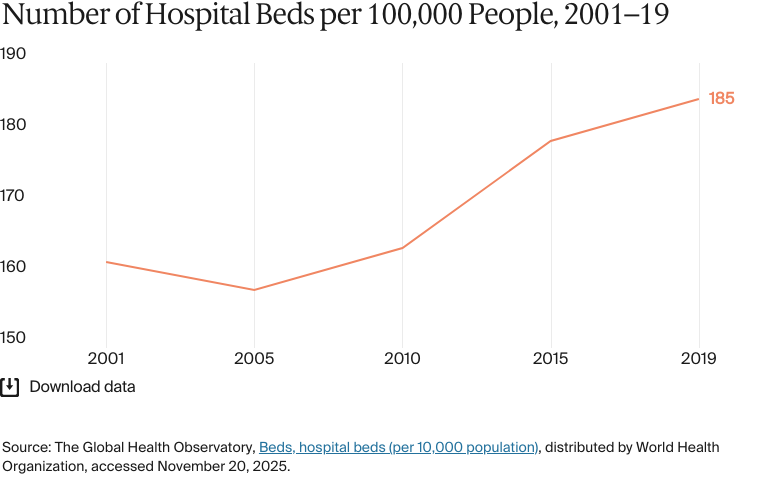
The hospital system is a mix of public, private, and charitable institutions, with oversight primarily provided by the MoHME. As of 2024, there were just under 1,100 hospitals, including 749 affiliated with the MoHME, 73 managed by the SSO, 32 operated by military organizations, 37 operated by charities, and 166 privately run.
Public hospitals offer more affordable care, with basic insurance covering a significant portion of inpatient and outpatient costs. Patients in private hospitals often face higher out-of-pocket expenses, sometimes paying up to 70 percent of the total cost unless they’re covered by supplementary insurance. The payment model in private hospitals typically follows a fee-for-service approach, applied per visit for outpatient care and per day for inpatient services.
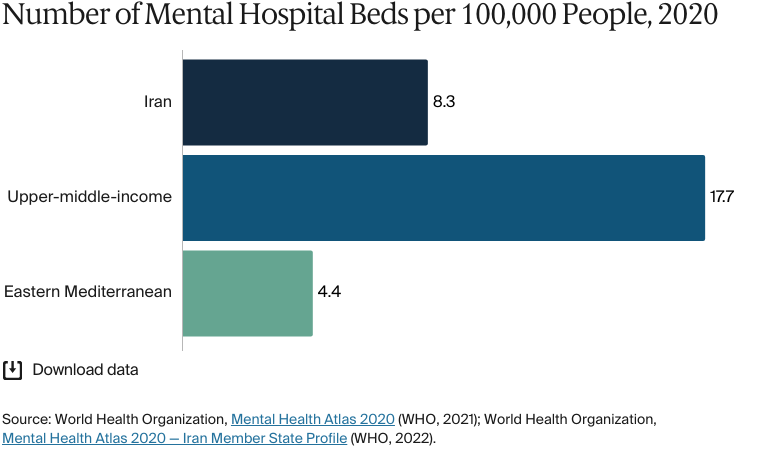
Mental health is a growing public health priority. An estimated one-fifth of the population has a mental health or substance use disorder, and these collectively account for nearly 10 percent of the national disease burden.
Mental health care was integrated into the primary care system in 1989. Initially targeting rural populations through screening and referral protocols embedded in khaneh behdasht activities, integration efforts brought rural mental health access close to urban levels. However, over 60 percent of people with mental disorders receive no care, and only 15 to 25 percent receive appropriate clinical treatment.
Services are delivered through a combination of psychiatric hospitals, outpatient clinics, private practices, and community mental health centers (CMHCs). CMHCs provide walk-in and referral-based outpatient psychiatric care, structured follow-up for severe cases, and continuity of care through insurance-backed services.
The Comprehensive Mental and Social Health Services initiative (SERAJ) aims to provide integrated care across three levels: mental health screening and counseling in primary health care centers, specialized treatment through CMHCs and psychiatric hospitals, and community-based social support initiatives. The program also promotes intersectoral collaboration with the ministries of welfare, education, and labor to support social reintegration and protection for marginalized individuals.
To improve financial protection, a national fund was introduced in 2022 to support individuals with severe mental illnesses and incurable diseases. Administered by the health insurance and social security agencies, the fund exempts eligible patients from hospitalization deductibles and is linked to updated accreditation standards for psychiatric care facilities.
Long-Term Care and Social Support
The long-term care system is characterized by a combination of institutional facilities, limited community-based services, and a reliance on informal, family-provided home care. Despite the aging population, the long-term care infrastructure is underdeveloped and lacks standardized eligibility criteria, integrated care pathways, and comprehensive insurance coverage. The distribution of community-based services for elderly care is sparse and mainly targeted at people with disabilities.
Institutional Care
Institutional long-term care mainly consists of nursing homes and rehabilitation centers managed by the State Welfare Organization (Sāzmān-e Behzisti-ye Keshvar) These facilities aim to provide educational, rehabilitation, and recreational services. However, many fall short in addressing the specific physical and emotional needs of the elderly, often lacking age-appropriate infrastructure and adequate psychological and social care provisions. Consequently, Iranians have a negative perception of nursing homes, which are seen more as temporary shelters than as supportive environments for aging individuals.
Home-Based and Informal Care
Home-based care is the most prevalent form of long-term care and is heavily dependent on informal caregivers — typically family members. This reliance is rooted in cultural norms and the absence of formal home care services. Without any substantial support from the health care system, informal caregivers often struggle with a lack of training, financial strain, and emotional stress.
Community-Based Services
Community-based long-term care services are limited and mainly supported by local initiatives that provide basic health services and support for the elderly within the community. However, the scale and reach of such programs aren’t enough to meet growing demand.
Policy and Financial Framework
There’s no formal long-term care insurance system. Financing for long-term care is fragmented, with costs shared between public funds and private out-of-pocket payments by families. The State Welfare Organization’s Empowerment of the Elderly program offers some in-kind support, such as rehabilitation equipment and fee exemptions, for low-income seniors requiring institutional care. However, these measures are limited in scope and don’t constitute a comprehensive financial protection mechanism.
Strategic Initiatives
To meet the challenges of an aging population, the government has initiated such strategic programs as:
- The National Plan for Older Persons (Sanad-e Melli-ye Sālmandān), a policy framework for coordinating efforts across sectors to improve health, social supports, and financial security
- The Age-Friendly Environment initiative (Mohit-haye doostdar-e salmand), which was launched in partnership with the United Nations Population Fund to create supportive environments that promote active aging and community participation.
However, addressing significant shortcomings in the provision of comprehensive, accessible, and high-quality long-term care services will require more, including the introduction of integrated care models, formal home care services, and sustainable financing mechanisms.
Cost and Affordability
Health Care Spending Overview
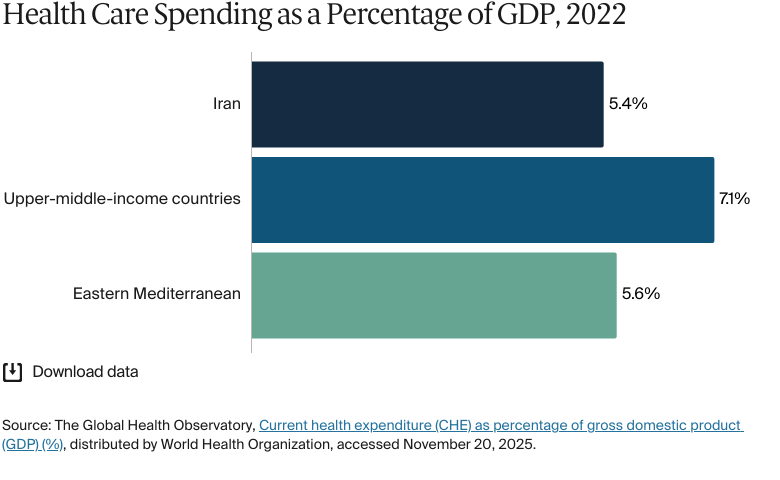
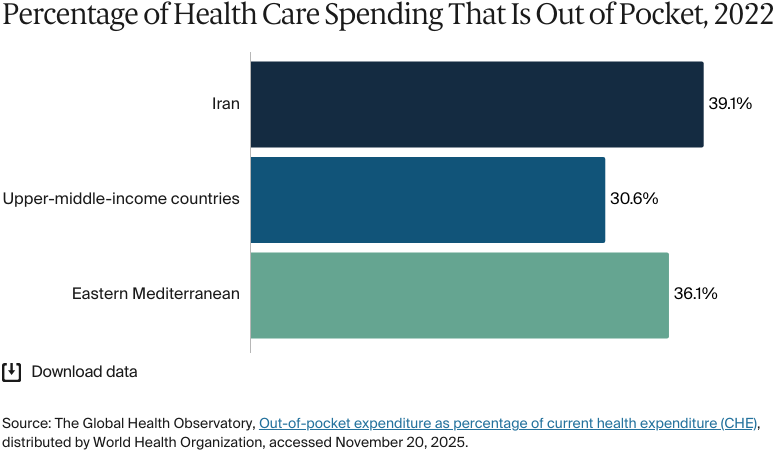
In 2023, about 6 percent of gross domestic product (GDP) was spent on health care, lower than the 7.1 percent average for upper-middle-income countries.
In 2022, total health expenditure was USD 19 billion, with an average of USD 221 spent per person. Public funding sources — including government budgets and basic health insurance plans — covered 55.5 percent of this expenditure, and out-of-pocket payments were 33.9 percent.
The HTP aimed to reduce household contributions and expand access to subsidized services. Although there have been some improvements, particularly in access to public hospitals, persistently high out-of-pocket payments suggest that many services, especially in the private sector and for outpatient care, still aren’t adequately covered by insurance (see Cost Sharing and Out-of-Pocket Spending).
Efforts to improve the efficiency and equity of health financing have focused on increasing strategic purchasing, revising insurance benefit packages, and boosting targeted subsidies for low-income groups. However, constrained fiscal space and sanctions continue to limit the government’s ability to expand public investment in health.
International sanctions have reduced access to health care. They have led to a one-third decrease in public purchasing power to cover health expenditures, triggered shortages of 73 medications (44% of which are classified as essential by the WHO), and limited access to treatments for some 6 million people.
Pharmaceutical Spending
In 2024, the pharmaceutical market is projected to generate about USD 8 billion in revenue. Pharmaceutical costs are shared among stakeholders through a structured copayment model: individuals contribute 20 percent, insurance funds cover 45 percent, and the MoHME subsidizes the remaining 35 percent (specifically for the lowest-priced generics).
The National Pharmaceutical Policy (Siasat-e Melli-e Darouyi-e Iran), governed by the IFDA, emphasizes accessibility, affordability, and reduced dependency on imports, with a strong preference for locally produced generics. However, the system faces challenges due to subsidy leakage, limited benefit package coverage for newer high-cost biologics, and fragmentation across multiple stakeholders (the MoHME, the IFDA, insurers, and parliament). High-tech imported drugs, such as monoclonal antibodies and advanced oncology treatments, are largely unaffordable and are often excluded from public reimbursement programs.
Cost Sharing and Out-of-Pocket Spending
Out-of-pocket payments made up 43.15percent of total health expenditures in 2023 — a significant financial burden on households. In 2021, 0.1 percent of Iran’s population was pushed below the poverty line of USD 1.90 per day because of household health expenditures.
During the COVID-19 pandemic, pharmaceuticals accounted for 45 percent of total direct health care costs. Patients were responsible for 57 percent of these expenses.
For long-term care services, which are not covered by basic health insurance or supplementary plans, patients pay an average of 39 percent out of pocket.
How Are Costs Contained?
The Family Physician Plan (Barnameh-ye Pezeshk-e Khanevadeh), scheduled for nationwide implementation in 2025, aimed to strengthen primary care services and establish a structured referral system. By promoting initial diagnosis and treatment at the primary care level, the plan seeks to reduce unnecessary specialist visits and minimize costly interventions. Patients adhering to the referral pathway benefit from significantly reduced expenses, including zero tariffs for basic services, such as consultations and paraclinical exams, and no deductibles for hospitalization in public facilities.
The health technology assessment complements this. It evaluates the clinical effectiveness and cost-efficiency of medical technologies and interventions to make sure that health resources are allocated where they offer the highest value. Integrating the health technology assessment into policymaking is designed to guide investment decisions with evidence and prioritize interventions that deliver substantial health outcomes per unit cost.
Quality and Outcomes
Health Outcomes
In 2023, life expectancy was 78.8 years, compared with 73.7 years in North Africa and the Middle East. Life expectancy was 80.6 years for women and 77.2 years for men.
In 2021, the leading cause of death was noncommunicable diseases, accounting for 56.8 percent of all deaths. This was followed by communicable, maternal, perinatal, and nutritional conditions at 29.4 percent, while COVID-19-pandemic-related outcomes accounted for 7 percent, and injuries made up the remaining 6.8 percent.
Addressing Health Inequities
Despite broad coverage goals, there are persistent inequities in Iran’s health system. Although socioeconomic inequity in accessing inpatient services decreased following the implementation of the country’s HTP, socioeconomic inequities in accessing outpatient services still exist, mainly due to members of higher socioeconomic groups being able to purchase supplementary health insurance. The burden of catastrophic health expenditure is not equitably distributed and disproportionately affects poorer households.
Geographical inequities are also apparent. Modeling in Sistan and Baluchestan Province (a province with a large population of Baloch people, who are an ethnic minority in Iran) finds significantly lower spatial accessibility to facilities compared with better-served areas. This is particularly prominent in more rural areas of the province. Nearly 75 percent of the population has low/no access to overall primary care services within a 30-minute drive.
The United Nations Committee on the Elimination of Racial Discrimination has documented structural discrimination against ethnic and ethno-religious minorities in Iran. Discrimination is particularly prevalent in minority–majority provinces, where minority groups may face additional barriers to accessing health services and report poor health outcomes, such as higher infant mortality.
There are also gendered barriers. Male-guardianship-related constraints can hinder women’s access to health services and social security, while recent policy changes designed to boost Iran’s population have banned free access to contraception and made abortion illegal.
Refugees and migrants benefit from Iran’s Universal Public Health Insurance (Bimeh-e Salamat-e Hamgani), but coverage depends on documentation, and recent studies identify gaps and barriers to care.
People with disabilities face non-financial barriers (time, geography, physical access, acceptability) and socioeconomic obstacles that limit service use.
Several community-based initiatives aim to mitigate inequities in Iran’s health care system. One is the Barakat Foundation’s (Bonyād-e Barekat) Back to the Village (Bāzgasht be Rustā) plan, which aims to reverse rural-to-urban migration by creating sustainable job opportunities in villages and enhancing access to local health and social services. Another is the Read with Me project launched by Iran’s Institute for Research on the History of Children’s Literature (Mu'asseseh-ye Pazhuhesh dar Tārīkh-e Adabiyāt-e Kūdakān) to promote literacy among disadvantaged children, particularly those living in remote areas or working on the streets. It is hoped that fostering early education in this way will support better futures, including long-term health outcomes.
Ongoing strategies that focus on improving health literacy, expanding access to essential services, and addressing the social drivers of health will continue to be crucial for making health outcomes equitable for all populations.
Innovation and Reform
Health Care Innovation
The HTP introduced comprehensive reforms aimed at enhancing access, equity, and financial protection within the health care system. Results so far have been mixed: early phases reduced inpatient out-of-pocket payments in public hospitals and expanded insurance coverage. However, out-of-pocket costs have risen in many settings, while patient satisfaction has declined.
Important initiatives under this program include:
- The Ghasedak Plan. Implemented in 2015, this introduced a performance-based payment system for nonphysician hospital staff, linking compensation to performance. Success has been limited by inadequate information infrastructure — particularly in rural areas and within the family physician program, where insufficient internet access and the lack of necessary software and hardware affect monitoring and evaluation.
- Improvement of hospital services. A focus on enhancing the quality of hospital services, commonly referred to as “hoteling,” has upgraded hospital infrastructure, improved cleanliness, and enhanced patient amenities to increase patient satisfaction and trust in public health care facilities.
- Enhancement of emergency medical services. The HTP has strengthened emergency medical services by expanding air ambulance services and improving the responsiveness of emergency departments. This has helped to reduce mortality rates and improve functional outcomes for patients in rural areas.
- Strengthening primary health care infrastructure. The HTP has emphasized reorganizing and upgrading primary health care services, especially in underserved areas. This included the development of khaneh behdasht and rural health centers as well as the recruitment of health teams to provide comprehensive services. Preventive measures for noncommunicable diseases have been integrated across age groups.
Health Care Technology
There has been progress in the use of digital technologies to strengthen health care, particularly in response to the COVID-19 pandemic. In 2020, telemedicine services were launched across six provinces and 23 underserved areas, facilitated through national hotlines. Online consultations were carried out on platforms such as Imam Khomeini Hospital’s virtual clinic and Paziresh24 and using mobile applications such as Snapp and Mask. The Mask app played a role in enabling smart quarantine and minimizing exposure in crowded areas. Additionally, nongovernmental organizations supported cancer care through the hotline 4030 by offering virtual counseling services and training volunteers in cancer management.
The national electronic health record (EHR) system (Samaneh Parvande Electronic Salāmat, or SEPAS), was launched in 2007 to integrate patient data from hospitals nationwide. It collects demographics, diagnoses, procedures, lab results, and billing data via decentralized nodes linked through a secure network. SEPAS has been criticized, however, for its system instability, limited clinical adoption, lack of integration with mobile and other devices, and minimal impact on improving patient care and reducing paperwork.
An integrated EHR system focusing on primary care, known as SIB, was implemented in 2015. It has been deployed in more than 36,000 urban and rural health centers and involves more than 130,000 health care workers. Along with SinaEHR, another primary care EHR system, SIB feeds point-of-care data into SEPAS.
Additionally, innovative efforts, such as a low-cost, internet-based heart monitoring using cloud computing and machine learning, are being piloted to enhance rural care delivery. As of 2023, EHRs have been created for about 98 percent of the population — a milestone in digital health coverage.