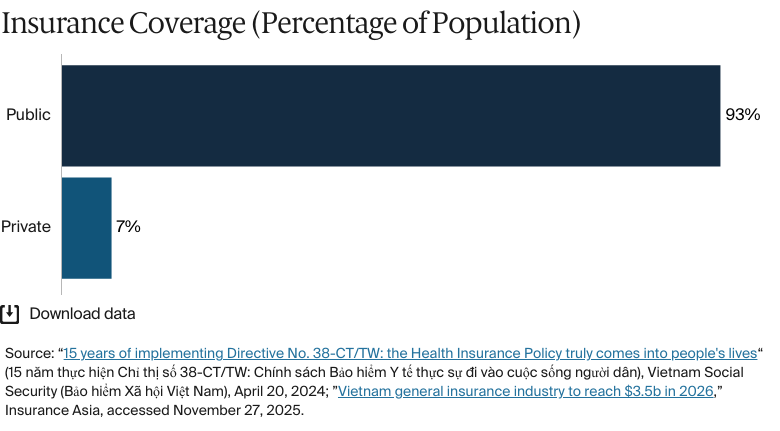
Vietnam’s health care system has expanded rapidly over the past 15 years and now covers 93 percent of the population. It’s funded by contributions from employers, individuals, and the government. The system is divided into two strands: free health care, available to war veterans and economically disadvantaged groups, and public health insurance, available to the majority of residents, who have to make copayments. As a result of its expanded health care system, Vietnam has made strong progress in combating infectious diseases such as HIV/AIDS, malaria, and tuberculosis.
However, for many people in Vietnam, the financial burden of health care is high. About 40 percent of total health care spending is out of pocket, approximately the same as the percentage spent by the government. Strategies to increase the availability and affordability of health care include expanding the rollout of telemedicine and establishing public-private partnerships to improve hospital infrastructure and services.
In Vietnam, the health system is divided into two streams: free health care for war veterans and economically disadvantaged groups, and social health insurance, which is available to the majority of the rest of the population. All citizens employed for more than three months, civil servants, people with disabilities, and veterans are automatically enrolled in compulsory social health insurance schemes while self-employed or informal workers are able to opt into voluntary schemes.
Public insurance coverage: 93% of population
Private insurance coverage: 7% of population
Primary care physicians: Not available
Specialist physicians: Not available
In 2022, government spending accounted for 43 percent of health expenditure, prepaid private spending made up 16 percent.
Out of pocket spending: 39.4% of total health care spend
A ten-year gap exists in life expectancy between men and women in Vietnam, and significant outcome disparities exist for populations in rural and remote areas, as well as among Hmong and Thai ethnic groups, where maternal mortality rates are particularly high.
Before 1945, under French colonial rule, Vietnam lacked formal health insurance. Instead, the nation relied on traditional community support networks. The period from 1945 to 1975 saw the establishment and expansion of social health insurance (SHI) under the Democratic Republic of Vietnam.
Since the 1980s, Vietnam has transformed from one of the world’s poorest countries to a lower-middle-income economy. In 1986, a set of policies known as the Đổi Mới (Doi Moi, or “renovation”) changed Vietnam from a command economy to one based more on market economics.1
The country has made significant progress in improving the capacity of its health service and the health workforce, according to Angela Pratt, the World Health Organization (WHO) representative in Vietnam. Combined with the expanding reach of Vietnam’s health system, that progress contributed to the country’s strong response to the COVID-19 pandemic.
Vietnam has also made strides in reducing the infectious disease burden.
In the past decade or two, Vietnam has made incredible progress in almost controlling diseases such as HIV, and it is very close to eliminating malaria. It has also made impressive progress in reducing the incidence of tuberculosis.
Angela Pratt
Representative in Vietnam
World Health Organization (WHO)
The Role of Public Health Insurance
Vietnam aims to provide universal health coverage through its SHI system. All citizens employed for more than three months, civil servants, people with disabilities, and veterans are automatically enrolled in compulsory SHI programs. Self-employed or informal workers can opt into voluntary SHI programs.2
More than 93 percent of Vietnam’s population was covered by public health insurance in 2023, compared with 58 percent in 2009. This increase is attributed to a government directive aimed at improving the implementation of health insurance policies.3
According to the WHO’s Angela Pratt, the government has invested significantly in the system, and that investment is underpinned by comprehensive policy frameworks and institutional support.
However, SHI is still a work in progress. Pratt says that the program doesn’t always provide enough financial protection, meaning out-of-pocket costs are still quite high. Typically, people with SHI are covered for up to 80 percent of health care costs, with a 20 percent copayment.4
Inpatient care, fully covered at commune-level hospitals
Outpatient care, fully covered at commune-level hospitals.
Services that have limited coverage include:
Necessary dental care, such as tooth extractions
Basic eye care
Mental health care
Assistive devices, such as prosthetics and wheelchairs.
Services not covered include:
Home visits
Palliative care
Long-term care.
Safety Nets
The Law on Health Insurance gives all health insurance enrollees coverage for medical exams, treatments, rehabilitation, prenatal check-ups, childbirth, and patient transport from the district level to higher levels.6
Low-income households, people over age 80, and children under age 6 are fully covered under SHI.7 Other groups that receive 100 percent coverage include members of ethnic minority groups living in disadvantaged areas, retired workers, and recipients of certain social and disability allowances.8
Vietnam has tried to strengthen its health care safety net by identifying people who might be overlooked by the current system, such as workers in the informal sector or people in remote locations. Uninsured people with tuberculosis are another overlooked group. In 2022, tuberculosis services were integrated into SHI as part of a broader effort to increase domestic state financing for health care. This integration, however, means that patients must use SHI for treatment at district-level facilities; those who don’t must pay for services out of pocket.9
The Role of Private Health Insurance
Commercial health insurance, which does not replace SHI, includes private coverage that companies offer to their employees.10
There are no data available for the percentage of the population which uses private health insurance. But enrollment has increased in recent years, particularly among urban and higher-income groups, as disposable income has increased.11
The Role of Government
Vietnam Social Security (VSS; Bảo hiểm Xã hội Việt Nam) is the government agency responsible for implementing SHI, overseeing related funds, and handling the insurance premium collection process through approved service organizations.
VSS contracts with medical providers to deliver insurance-covered services; it supervises these contracts and ensures the protection of enrolled individuals. The agency has statutory responsibility for managing and using insurance funds transparently, implementing approved investment plans, and managing investment risks.12
Integration and Care Coordination
Vietnam’s government has used public-private partnership (PPP) models to bridge gaps between investment needs and state financing capacity. However, the use of PPPs in health care is limited: in 2020, 63 potential PPP projects were considered, but by August 2024, only two of these had been completed.13 Most proposed PPPs focus on urban hospital infrastructure and services rather than on preventive and primary health care (among the most pressing needs) or on health care resources for lower-income groups in rural areas.
Other initiatives seek to address Vietnam’s changing health needs, from acute care to the management of noncommunicable diseases and chronic conditions. A pilot project run by the Ministry of Health (MOH; Bộ Y tế) and the National Institute of Hygiene and Epidemiology (Viện Vệ sinh dịch tễ Trung ương), partially supported by the WHO, has been improving the management and treatment of noncommunicable diseases in Ho Chi Minh City. Since the pilot’s inception in 2022, the initiative has supported 10 of 22 district health centers and 43 of 310 commune health stations to integrate the management and treatment of noncommunicable diseases into primary health care. There are now plans to expand the program to health stations and health centers across the country.14
An MOH initiative designed to improve the management of noncommunicable diseases in the community had been implemented at 68 health stations in 14 districts across seven provinces by November 2022.15 In addition, more than 350 health workers had been trained in the community management of these diseases.16
Operations and Resources
Overview of the Delivery System
Vietnam’s health care system is a tiered structure that provides a range of services across various levels of care. The system can be broadly categorized into the following groups:
Primary care is typically the first point of contact for patients provided at commune health stations and by village health workers. Services include general practice, vaccinations, maternity care, basic mental health support, and health education programs.
Secondary care includes planned or elective medical services provided at district and provincial hospitals. Secondary care includes inpatient and outpatient care, diagnostic services, treatment for less complex conditions, and urgent and emergency care.
Tertiary care includes specialized treatments offered at national and specialist hospitals and managed by the MOH. Services include complex surgeries, advanced diagnostics, and treatment for rare or severe diseases.
Since 2014, there have been three payment models for health providers in Vietnam: capitation, fee-for-service, and diagnosis-related group payments. Fee-for-service payments are the most commonly used, despite the risk of care delivery fragmentation and cost escalation. Health care providers receive budget funding, payments from VSS, and payments from patients.17
Primary Care
Primary health care in Vietnam covers 10 main areas:
Illness treatment and prevention
Health education
Local disease control
Immunization
Maternity care and health care for children
Essential medicines
Nutrition
Clean water and environmental sanitation
Health management
Strengthening the grassroots (community-based) healthcare network.18
In 2022, Vietnam had 100 doctors for every 100,000 people, compared with 77 in lower-middle-income countries.19 There are no data available for nurse and pharmacist numbers.
Within primary care settings, village health workers play a critical role — especially in underserved rural areas. These workers receive specific training to allow them to volunteer in the community, provide basic health care and counseling, and act as links between residents and their commune health centers. In 2020, Vietnam had nearly 98,000 village health workers.20 In a number of community-based health centers, services such as immunizations, hygiene and nutrition guidance, and maternal care and childcare are often provided free or at very low cost.21
Vietnamese citizens are not required to register with a primary care practice.
Physicians and village health workers are not required to provide out-of-hours care to their patients. Some commune health centers offer some primary care services at night or on weekends, but their capacity is limited compared with larger hospitals. Typically, such care is handled by district or provincial hospitals, which provide 24/7 emergency services.
There are no data available for the proportion of primary care physicians employed privately versus publicly.
Outpatient/Specialist Care
Outpatient specialist care is provided by a mix of public and private hospitals, which are typically located in major cities, and by specialist doctors (levels 1 and 2). Level 1 doctors have received two years of specialist training and one year of orientation after graduating from medical school.22 They can then undertake further training to reach level 2, equivalent to a master’s degree in medicine.
There are no data available for the number of specialist physicians in Vietnam or for the proportions who work in public or private practice.
Physician Education and the Workforce
The government can train 13,000 medical graduates per year. On this basis, Vietnam’s goal is to achieve 150 doctors for every 100,000 people by 2025. This plan is part of a government decision, signed in March 2024, that approved the country’s health network planning for 2021–30, looking ahead to 2050.23
The cost of attending medical school in Vietnam varies by university, but it is affordable when compared with costs in other countries. On average, students pay between USD 5,000 and USD 8,000 a year.24 Despite their relative affordability, these fees remain out of reach for the majority of Vietnamese students, as the average annual household income per capita is about USD 2,410.25
Despite these relatively low education costs, Vietnam has a significant shortage of primary care preventive medicine workers who focus on preventing illness rather than treating it. In 2022, it was estimated that the country needs a minimum of 24,000 additional preventive medicine workers, including 8,000 doctors and 4,000 public health workers with bachelor’s degrees.26
There are also shortages of qualified physicians in rural areas. Vietnam’s government has issued several decrees aiming to improve financial incentives for rural health workers. For example, health workers in rural areas are now eligible for an additional 70 percent of their basic salary during their first five years of service.27
In some rural areas, doctors receive higher incomes as well as housing subsidies. Another government decree states that after three years of rural service, health workers can be promoted to civil servant positions. Because these positions are highly regarded, this policy could incentivize health workers to pursue careers in rural locations.28
Hospitals
Both public and private hospitals play a role in health care delivery in Vietnam. Public hospitals are primarily owned and operated by the government, with oversight from the MOH and provincial health departments.
Private hospital numbers have increased over the past decade, partly due to government policies that encourage private investment in health care.29 In 2025, there were about 400 private hospitals.30
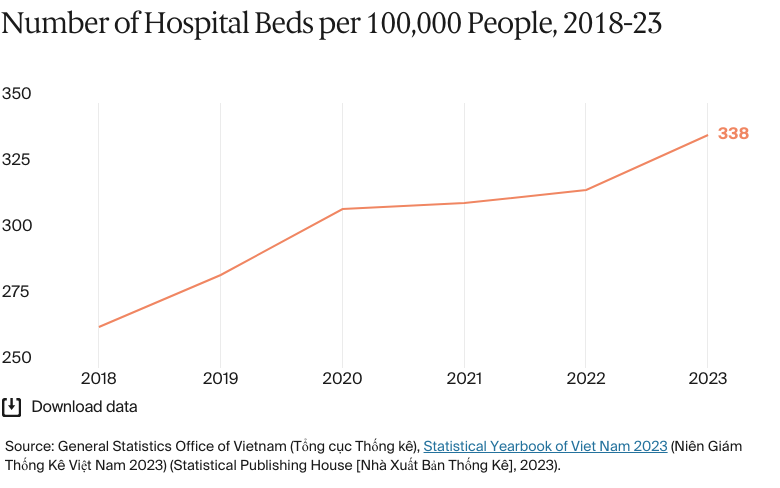
Vietnam had about 338 hospital beds for every 100,000 people in 2023.31 There are no data available for the number of nurses and pharmacists.
Mental Health Care
BY THE NUMBERS
In 2021, there were 0.6 psychiatrists per 100,000 people, compared to an average of 0.4 for lower-middle-income countries.32
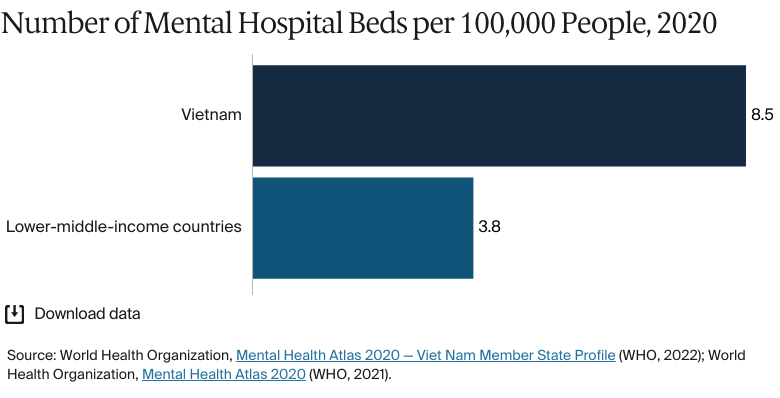
In 2020, there were nine mental hospital beds per 100,000 people, higher than the average of four for lower-middle-income countries.33
In 2020, there were 4.2 mental health professionals per 100,00 people, nearly the same as the average of 3.8 for lower-middle-income countries.34
In 2021, the prevalence of the Vietnamese population with mental health disorders was 10.1 percent, compared with an average of 13.5 percent in lower-middle-income countries.35
There were 4.2 mental health professionals for every 100,000 people in Vietnam in 2020, compared with an average of 3.8 in lower-middle-income countries.36 In 2022, a survey carried out by the Department of Medical Examination and Treatment Management found that 61 percent of district hospitals and health centers provided outpatient mental health care. However, only 9 percent provided inpatient mental health care, highlighting a significant gap in mental health treatment at the district level.37
Vietnam’s National Strategy on Mental Health for 2016–25 aims to improve mental health, prevent mental health conditions, and ensure equitable and effective medical and social care services.38 The strategy’s vision extends to 2035, and it focuses on:
Strengthening leadership, administration, and intersectoral cooperation
Enhancing comprehensive, integrated, and community-based health and social services
Improving mental health and preventing disorders
Innovating and improving health and social care and moving toward fairness, efficiency, and quality
Strengthening the capacity and effectiveness of mental health resources related to the prevention, detection, treatment, and management of mental illnesses, as well as rehabilitation and social support
Enhancing the evidence base about and research into mental health.
In response to increasing mental health challenges, the government is focusing on promoting social work and counseling positions in medical and educational facilities.
Long-Term Care and Social Support
Vietnam has one of the fastest-growing aging populations in Asia.39 People age 65 and over made up 9 percent of the total population in 2022 and are set to reach 20 percent by 2050.40
Long-term care is either community- or family-based or provided in institutional settings. Community- and family-based care includes home-based care provided by volunteers and intergenerational self-care clubs. This model combines preventive services, chronic disease management, and social support aimed at improving the quality of life of older adults. Institutional care is delivered in social welfare centers and private care centers for the elderly.41
On average, the lowest cost per resident for nursing homes providing comprehensive health care for the elderly is about VND 7 million (USD 276) a month. This fee fluctuates depending on the health condition, and additional health care services packages can cost up to about VND 15 million (USD 591) a month.42 The average monthly salary is about VND 8.5 million (USD 335), so the cost of comprehensive private nursing care is out of reach for most Vietnamese people.43
The Asian Development Bank (ADB), which provides funding and technical assistance for health care projects across Asia, has five recommendations to address the cost of long-term care in Vietnam.44 While these recommendations offer a road map for strengthening the long-term care system, Vietnam’s progress in adopting these measures remains a work in progress:
Preventing disease and frailty: The ADB emphasizes the need to prevent and manage noncommunicable diseases and accidents and to promote health. Vietnam has introduced several noncommunicable disease prevention programs, but scaling these efforts and addressing gaps in rural areas remain challenges.45
Enhancing accessibility to health care: The ADB advocates for improved access to affordable assistive devices, home modifications, and age-friendly communities. Vietnam has initiated policies to support disability-inclusive care and infrastructure development, but affordability and widespread access are still barriers for many.
Increasing support for family carers: The ADB suggests providing training and social protection for family carers. While Vietnam recognizes the role of family carers, formalized support structures, such as training programs and financial assistance, are still limited in scope.
Expanding the role of volunteers: The ADB recommends integrating trained volunteers into home- and community-based care. Vietnam has piloted community-based volunteer programs in some regions, though further integration into health services and consistent training remain areas for improvement.46
Integrating long-term care services into existing health and social care systems: The ADB highlights the importance of embedding long-term care within existing health and social systems to reduce redundancy and costs. Vietnam is exploring how to leverage its current infrastructure and policies, but comprehensive integration and sustainable funding mechanisms have yet to be fully realized.
Cost and Affordability
Health Care Spending Overview
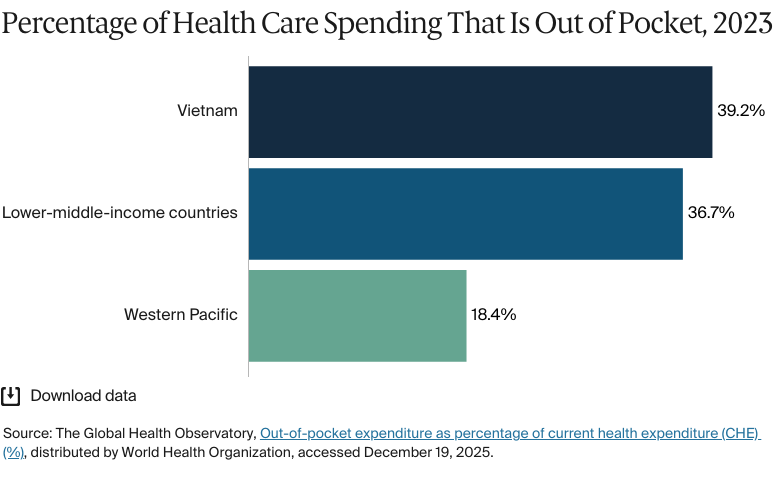
In 2022, the government was responsible for nearly half (43.4%) of overall health care spending in Vietnam, followed closely by out-of-pocket spending at 39.4 percent (the same for 2023, see Cost Sharing and Out-of-Pocket Spending). Prepaid private health care spending accounts for 15.6 percent, while funding from international development agencies accounts for 1.6 percent.47
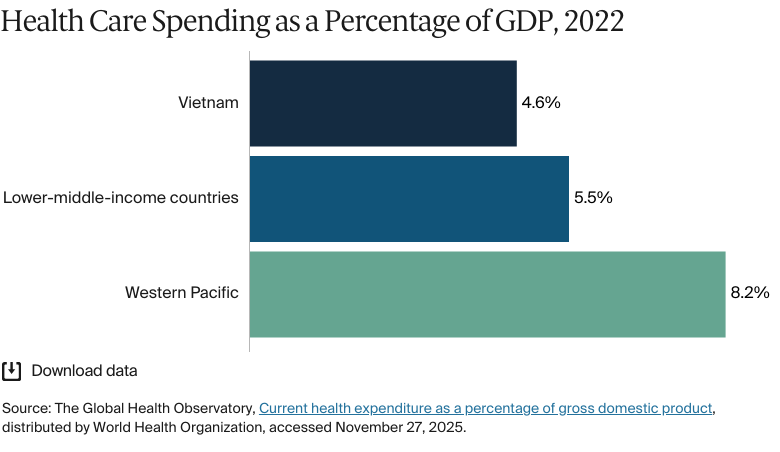
Vietnam’s total all-cause spending has increased from USD 8.9 billion in 2010 to USD 17.2 billion in 2021.48 However, Vietnam’s health expenditure as a percentage of gross domestic product (GDP) has decreased since 2010 and is lower than the average for lower-middle-income countries.49
Pharmaceutical Spending
In 2022, the average spending on pharmaceuticals per capita was about VND 1.9 million (USD 75). This is a significant increase from previous years: in 2015, the average spend was only about VND 1 million (USD 38).50 There are no data available for the percentage of the health care budget spent on pharmaceuticals.
Increased spending on pharmaceuticals does not always make them easier to access. Less than 10 percent of new drugs (those entering the global market between 2012 and 2021) were available in Vietnam in 2022. There are also difficulties accessing generic drugs. The proportion of generic drugs used in Vietnam’s medical facilities is just 11 percent, compared with the Asia-Pacific average of about 27 percent.51
The Drug Administration of Vietnam, responsible for all drug approvals, plans to leverage legal changes to streamline processes and provide incentives for international pharmaceutical companies looking to distribute their products in the country, with the aim of improving patient access to treatments.52 The agency also plans to enhance Vietnam’s pharmaceutical manufacturing capabilities and make the country a high-value regional center by 2030.53
Cost Sharing and Out-of-Pocket Spending
Out-of-pocket spending accounts for nearly the same percentage of total health expenditure as government spending, an indication of the high financial burden that health care places on Vietnam’s population.
Patients face higher copayments if they skip the primary care referral process.54 Usual copayment rates for insured members range from 0 to 20 percent. Those who bypass the referral process face copayment rates of 30, 40, and 60 percent for district-, provincial-, and central-level providers, respectively.55
How Are Costs Contained?
Vietnam’s health care budget is decentralized, which means that local authorities have significant control over budget allocations. Authorities have the ability to levy local taxes and decide on the allocation of revenue and spending across local budgeting levels and functions, including health.56 Allowing local authorities to distribute their resources according to local need helps them invest efficiently and focus on the areas of greatest need.
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
Life expectancy at birth was 76.1 years in 2023, compared with 77.4 years for SouthEast Asia, east Asia and Oceania.57
Life expectancy for women was 80.2 years in 2023, the same as in SouthEast Asia, east Asia and Oceania.58
Life expectancy for men was 71.9 years in 2023, compared with 74.8 years for SouthEast Asia, east Asia and Oceania.59
The top three causes of death in 2021 were:
Stroke: 186 deaths per 100,000 people
Ischemic heart disease: 72 deaths per 100,000 people
Chronic obstructive pulmonary disease: 44 deaths per 100,000 people.60
The maternal mortality rate in 2023 was 48 deaths per 100,000 live births, compared with an average of 35 across Western Pacific countries.61
The infant mortality rate in 2023 was 14 deaths per 1,000 live births, compared with an average of nine deaths across Western Pacific countries.62
In 2021, the share of the population with mental health disorders was 10 percent, compared with 14 percent on average in lower-middle-income countries.63
The suicide rate in 2023 was 9.7 deaths per 100,000 population, compared with nine deaths per 100,000 population on average for lower-middle-income countries.64
Guns were responsible for 0.6 deaths per 100,000 people in 2023.65
2 percent of adults were affected by obesity in 2022, compared with 12 percent on average for lower-middle-income countries.66
Vietnam aims to provide universal health coverage for all its citizens and to ensure that everyone, regardless of income, can access quality health care. Average life expectancy in Vietnam has risen since the start of the century. In 2000, men lived on average 67.6 years, while female life expectancy was 76.1 years.67 However, by 2021, male life expectancy was 69.7 years, and female life expectancy was 78 years.
On average, women live nearly a decade longer than men. While this reflects a global trend, the gap in Vietnam is wider than the global average. There is no widely held theory on why this might be the case, but research suggests that lifestyle factors are one reason. For example, in 2015, 45 percent of Vietnamese men smoked, compared with just 1 percent of women.68
Socioeconomic factors can influence life expectancy in Vietnam. Research shows that life expectancy is more contingent on income level and education than on living conditions.69
Differences in the health care available across Vietnam’s regions are especially evident in areas such as staffing, health budget allocation, and the availability of medical facilities — particularly in provincial hospitals. The Northern Midlands and Mountains region and the Central Highlands face significant challenges in improving service delivery and population health outcomes. Many of these challenges are due to a lack of infrastructure in these undeveloped areas.70
Maternal mortality rates also differ between regions and for certain minority groups, reaching up to 150 deaths for every 100,000 live births in some cases.71 In the Northern Midlands and Mountains region, for instance, Hmong and Thai women have an especially high maternal mortality rate.72
Despite some inequities in care, a relatively low proportion of the population says that they have unmet medical needs. Less than 2 percent of adults age 60 and over report an unmet need, a very low figure compared with some other lower-middle-income countries.73
Addressing Health Inequities
The vast majority of citizens now have SHI, but the WHO’s Angela Pratt says that it often doesn’t go far enough to address inequities. “People might be covered by SHI, but if it doesn’t cover enough of the cost of the service, it doesn’t help very poor inhabitants.”
The Vietnamese government is redesigning the health care system in an attempt to reduce the country’s health care disparities. Legislation passed in 2017 focused on restructuring health care financing to mobilize resources adequately and equitably, with an emphasis on improving the situation for marginalized populations, members of ethnic minority groups, and residents of remote, mountainous, border, and island areas. An amendment to the Law on Medical Examination and Treatment, also made in 2017, aimed to ensure that there are affordable medical services at all levels. This law provides a legal foundation for reducing health inequities.74
A United Nations Population Fund program has been established to reduce maternal mortality among ethnic minorities in Vietnam’s six most disadvantaged provinces. The program aims to:
Expand access to sexual and reproductive health services, including through telehealth
Improve emergency obstetric care capacity in remote locations
Create a village-based birth attendant network in remote locations
Increase health education and community mobilization.75
Innovation and Reform
Health Care Innovation
Since the establishment of VSS in 1995 and its consolidation of health insurance administration in 2002, reforms have focused on expanding universal health coverage, improving health care quality, and integrating digital health initiatives.76
In January 2024, the deputy prime minister signed a decision approving the national health strategy; this covers the period to 2030 but looks forward to 2045.77
The strategy’s goals for 2030 include the following:
Better disease prevention, particularly for emerging infectious diseases, health security, and readiness for climate change and public health emergencies. The strategy focuses on controlling risk factors and managing noncommunicable and occupational diseases.
Improved health service networks at all levels, narrower health disparities, and increased use of PPPs.
Special attention to maternal and child health, especially in ethnic minority communities and disadvantaged areas. The strategy focuses on training and deploying health care workers in rural and underserved areas.
The prioritization of scientific research and the application of advanced technology in disease prevention, diagnosis, and treatment. Emphasis is placed on employing digital technology to enhance health management and service delivery.
Access to quality medicines, vaccines, and medical supplies at reasonable prices. The strategy aims to increase public health expenditure, improve resource allocation, and achieve universal health insurance coverage. It prioritizes improvements to preventive medicine and health care in disadvantaged regions.
Looking ahead to 2045, Vietnam aims to meet diverse health care needs by attaining levels of innovation and integration comparable to those of high- and middle-income countries in the region.78
To achieve these overarching goals, a Health Care Network Planning strategy was approved with a scope until 2030, with the following developmental goals:
To build a national network of medical facilities to enhance health protection and care, aiming for equity, quality, efficiency, and international integration
To develop a network of medical examination and treatment facilities that meet health care needs, with each region having a general hospital and specialized centers
To upgrade provincial specialized hospitals, create high-tech hospitals that meet international standards, improve the out-of-hospital emergency system, and expand the number of high-tech private hospitals
To establish central and regional disease control centers
To upgrade national testing institutes, create regional testing centers, and develop a national medical equipment inspection center
To improve professional capacity for medical, forensic, and psychiatric assessments and develop facilities for reproductive health and elderly care.79
Health Care Technology
Vietnam’s public health system remains largely paper-based, and there is a lack of information technology (IT) support. Digitalization is a priority, but it faces significant challenges, including outdated IT infrastructure, limited funding for new technologies, a shortage of skills, and a lack of protocols for integrating data across medical systems.80
Telemedicine
In June 2020, the MOH approved the Telemedicine Examination and Treatment project for 2020–25. As part of the project, 24 hospitals provide support for remote medical examinations and treatment.81
Another telemedicine initiative, Doctor for Everyone, introduced a smartphone app that gives local communities better access to health care services. The program has equipped telehealth function rooms in 75 highly marginalized communes with computers, webcams, microphones, and high-quality external speakers to enable remote medical consultation services.82
More than 3,000 healthcare workers have been trained in telemedicine services through the initiative, which is taking place in 10 provinces.83
Electronic Health Records
As part of the government’s electronic health records (EHR) implementation plan, approved in 2023, nearly two thirds of all medical facilities had adopted EHRS by November 2025.84
However, the investment needed to adapt existing infrastructure and software systems to accommodate EHRs remains a significant obstacle.85 There is also a shortage of qualified professionals with the skills to implement EHR systems in Vietnam’s hospitals. Other challenges include insufficient IT infrastructure and workforce capacity, a lack of data-sharing protocols, interoperability issues, and insufficient cybersecurity skills.
Regulation Needs to Evolve to Keep Up
Digital technology has enormous potential for Vietnam, says the WHO’s Angela Pratt. It can provide consultations and other services to people in rural and remote areas, and AI could be used for diagnostics and to connect patient data. However, she also recognizes that poorly designed AI could lead to misdiagnoses, and there is a risk of unequal access to the most advanced digital health products.
“There are many opportunities, but the biggest risk I see at the moment is that there’s not an especially mature regulatory framework,” says Pratt. “When implementing new technologies, we need appropriate checks and balances [to] allow Vietnam to take advantage of the opportunities they offer [while also mitigating] the risks.”
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Quan-Hoang Vuong et al., “Good budget or good care: the dilemma of social health insurance in Vietnam.” SAGE Open Medicine 9 (September 3, 2021),https://doi.org/10.1177/20503121211042512.
↩
Rachel Forse et al., “Towards universal health coverage in Vietnam: a mixed-method case study of enrolling people with tuberculosis into social health insurance,” Health Research Policy and Systems 22, no. 40 (April 2, 2024),https://doi.org/10.1186/s12961-024-01132-8.
↩
Chi M Nguyen et al., “How public health insurance expansion affects healthcare utilizations in middle and low-income households: an observational study from national cross-section surveys in Vietnam.” BMC Public Health 23, no. 624 (March 31, 2023),https://doi.org/10.1186/s12889-023-15500-6.
↩
9
Forse et al., “Towards Universal Health Coverage.”
↩
Ministry of Health, “Workshop on strengthening primary health care.”
↩
17
Tran Thi Mai Oanh et al., Sustainability and Resilience in the Vietnamese Health System (London School of Economics and Political Science / Partnership for Health System Sustainability and Resilience, March 2021), https://www3.weforum.org/docs/WEF_PHSSR_Vietnam_Report.pdf.
↩
Nguyen K Quan and Andrew W Taylor-Robinson, “Vietnam’s evolving healthcare system: notable successes and significant challenges.” Cureus 15, no. 6 (June 14, 2023),https://doi.org/10.7759/cureus.40414.
↩
Bharat Vasireddy, “MBBS in Vietnam fees: a comprehensive overview for aspiring medical students,” Aieraa Overseas Studies, November 14, 2024, https://aieraa.com/mbbs-in-vietnam-fees/.
↩
Anna Zhu et al., “Analysis of strategies to attract and retain rural health workers in Cambodia, China, and Vietnam and context influencing their outcomes,” Human Resources for Health 17, no. 2 (January 7, 2019), https://doi.org/10.1186/s12960-018-0340-6.
↩
Jie Cai, “A robust health system to achieve universal health coverage in Vietnam,” The Lancet Regional Health — Western Pacific 37, no. 100854 (August 2023), https://doi.org/10.1016/j.lanwpc.2023.100854.
↩
Long-Term Care for Older People in Viet Nam: The Current Scenario, and Next Steps Toward a Healthy, Aging Population, (ADB Briefs, no. 218, Asian Development Bank, July 2022), https://www.adb.org/sites/default/files/publication/811931/adb-brief-218-long-term-care-older-people-viet-nam.pdf; Phan Hong Van et al., “Older Persons and Long-Term Care in Viet Nam,” in Coping with Rapid Population Ageing in Asia, ed. Osuke Komazawa and Yasuhiko Saito (ERIA, 2021), 45–56. https://asean.org/wp-content/uploads/2022/04/Coping-with-Rapid-Population-Ageing-in-Asia.pdf
↩
Asian Development Bank, Long-Term Care for Older People.
↩
45
World Health Organization, “Caring for people with noncommunicable diseases.”
↩
46
Asian Development Bank, Long-Term Care for Older People.
↩
47
Institute for Health Metrics and Evaluation, Financing global health, distributed by IHME, accessed November 27, 2025, https://vizhub.healthdata.org/fgh/.
↩
48
Institute for Health Metrics and Evaluation, Financing global health.
↩
49
The Global Health Observatory, Current health expenditure.
↩
Nguyen Thu Ha et al., “Health insurance reimbursement to hospitals in Vietnam: policy implementation results and challenges.” Health Services Insights 14 (April 14, 2021),https://doi.org/10.1177/11786329211010126.
↩
56
Creating Budgetary Space for Health in Vietnam by Reforming Expenditure Planning and Pro-Health Taxation: A Synthesis Report (United States Agency for International Development, October 2022), https://pdf.usaid.gov/pdf_docs/PA00ZVP5.pdf.
↩
57
GBD 2023 Demographics Collaborators, “Global age-sex-specific all-cause mortality and life expectancy estimates for 204 countries and territories and 660 subnational locations, 1950-2023: a demographic analysis for the Global Burden of Disease Study 2023,” The Lancet 406 (October 2025): 1731–1810, https://www.thelancet.com/action/showPdf?pii=S0140-6736%2825%2901330-3.
↩
58
GBD 2023 Demographics Collaborators, “Global age-sex-specific all-cause mortality and life expectancy estimates for 204 countries and territories and 660 subnational locations, 1950-2023: a demographic analysis for the Global Burden of Disease Study 2023.”
↩
59
GBD 2023 Demographics Collaborators, “Global age-sex-specific all-cause mortality and life expectancy estimates for 204 countries and territories and 660 subnational locations, 1950-2023: a demographic analysis for the Global Burden of Disease Study 2023.”
↩
Institute for Health Metrics and Evaluation, GBD Compare, distributed by IHME, accessed November 27, 2025, https://vizhub.healthdata.org/gbd-compare/ (overall firearm mortality is aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm).
↩
Tuyet Thi Nguyen and Maurizio Trevisan, “Vietnam a country in transition: health challenges,” BMJ Nutrition, Prevention & Health 3, no. 1 (2020),https://doi.org/10.1136/bmjnph-2020-000069.
↩
69
Le V Hoi et al., “Remaining life expectancy among older people in a rural area of Vietnam: trends and socioeconomic inequalities during a period of multiple transitions,” BMC Public Health 9, no. 471 (December 17, 2009),https://doi.org/10.1186/1471-2458-9-471.
↩
70
Yikai Feng et al., “Progress towards health equity in Vietnam: evidence from nationwide official health statistics, 2010–2020,” BMJ Global Health 9, no. 3 (March 18, 2024):e014739,https://doi.org/10.1136/bmjgh-2023-014739.
↩
Nguyen Anh Dang and Thi Phuong Thao Nguyen, “Reducing health inequalities in Vietnam: implications for health in all policy.” Vietnam Journal of Social Sciences 64, no. 3 (December 2022):65–70,https://doi.org/10.31276/VMOSTJOSSH.64(3).65-70 .
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.