The Netherlands operates a universal social health insurance system that combines public and private elements. All residents (excluding certain populations, such as some foreign students, undocumented migrants, and asylum seekers) are required to purchase statutory health insurance from private nonprofit insurers, which are obliged to accept every applicant.1 The standard insurance package covers most health services and is supplemented by public health programs and voluntary additional insurance.
The health system is funded mainly by individual insurance premiums and payroll taxes, supplemented by government grants and out-of-pocket payments.
Health care expenditure per capita is higher than the average for high-income countries and Europe. The Netherlands is among the better-performing countries in Europe and the world for health outcomes, with a below-average avoidable mortality rate and a low level of unmet medical needs.2 An aging population and the related increase in the incidence of chronic conditions are increasing demands and financial pressures on the health system. Reported mental health disorders are more prevalent than in most of the European Union.3
The Netherlands operates a universal social health insurance system that combines public and private elements. All residents (excluding certain populations, such as some foreign students, undocumented migrants, and asylum seekers) are required to purchase statutory health insurance from private nonprofit insurers, which are obliged to accept every applicant. The standard insurance package covers most health services and is supplemented by public health programs and voluntary additional insurance.
Primary care physicians: 372 per 100,000 people
Specialist physicians: 133 per 100,000 people
In 2024, In 2024, government spending and compulsory statutory health care insurance funded most of that health expenditure (83.2%), and voluntary private payments made up 5 percent of total expenditure. In 2023, the largest share of total health expenditure was allocated to long-term care (29.1%), followed by outpatient care (27%) and inpatient care (22%).
Pharmaceutical spending: 7% of total health care budget
Out of pocket spending: 11.8% of total health care spend
In 2023, there was a three-year difference between the life expectancies of men (80.3 years) and women (83.3 years).
On average, men are two and a half times more likely than women to take their own lives. In the past decade, rates have been highest for people ages 40 to 59.
The Netherlands’ first national health insurance program, introduced in 1941, was based on Germany’s “Bismarck” hybrid model of public and private health insurance coverage within a framework of extensive government control.About two-thirds of the population was covered by public health insurance; more affluent people could choose private coverage or remain uninsured. In the 1960s, a social insurance system was introduced for long-term care.4
In the early 2000s, concerns about rising health care costs and long wait lists led to a major market-oriented reform.5 The Healthcare Insurance Act 2006 (Zorgverzekeringswet [Zvw]) merged the existing public and private insurance markets into a single universal social health insurance program underpinned by private insurance. This substantially altered the role played by the government: from one of direct control over most care services and prices to one focused on regulatory oversight, with private insurers and health care providers responsible for planning and delivering most day-to-day health services.6
The health care system now offers near-universal service provision based on four forms of coverage:
The Zvw, which requires all residents to purchase basic health care insurance (basisverzekering) that covers a government-defined benefits package.7
The Long-Term Care Act 2015 (Wet langdurige zorg [Wlz]) for long-term residential care. The Wlz works on a single-payer system and is managed regionally by health insurers.8
The Social Support Act (Wet maatschappelijke ondersteuning [Wmo]), which forms the basis of a tax-funded system for in-home social care services, and the Child and Youth Act 2015 (Jeugdwet), which covers care and support for children and adolescents.9
The Public Health Act 2008 (Wet Publieke Gezondheid [WPG]), which regulates public health initiatives and the control of infectious diseases (for example, the national vaccination campaign during the COVID-19 pandemic).10
The Role of Public Health Insurance
All people who live or work in the Netherlands must purchase basic health care insurance from their choice of private insurer. It is also compulsory for parents to take out basic health care insurance for their children, but children do not incur insurance premiums until age 18. Insurers are obliged to accept all applicants, and enrollees have the right to change their insurer each year.11 As of 2024, there were 20 health insurers, with the four largest covering about three-quarters of the market.12
The government determines which health care services are covered by the basic health care insurance (updated on an annual basis) that must be offered by all insurers to policyholders regardless of their age and health. The basic health care insurance package is comprehensive (see Services Covered by Public Health Insurance), but certain services, including adult dental care and physiotherapy, are excluded (except for certain chronic conditions). Specific coverage rules, conditionality, and access to individual health care providers can vary between insurers.13
Nearly everyone (99.9%) has basic health care insurance.14 The government has introduced measures to identify people without insurance; in 2023, there were about 28,500 such uninsured.15 Anyone who is uninsured or who doesn’t make the required payments will be fined and can have their premiums taken directly from their wages or social security benefits.16
Active members of the armed forces, who are covered by the Dutch Ministry of Defence, are exempt from purchasing statutory basic health care insurance.17 Undocumented migrants can’t purchase health insurance and are required to pay for most services out of pocket. If this is not feasible, payments to providers may be covered by the government, subject to conditions and regulations overseen by the National Health Care Institute (Zorginstituut Nederland [ZIN]).18 There is a separate coverage system for political asylum seekers that is slightly less comprehensive than the statutory basic health care insurance.19
Foreign students cannot buy statutory basic health care insurance if they are in the country purely to study; they must arrange private coverage (or coverage through the General or European Health Insurance Card systems if they come from the U.K. or European Union [E.U.], respectively). All foreign students are required to take out basic health care insurance with a Dutch insurer if they work or do an internship while studying.20
Individual premiums are determined by each health insurer and paid directly by the insured. Insurers can offer different health plans according to the specific services covered, but the premium levied for each plan must be the same for all enrollees, regardless of their age or health status. As of 2025, the average annual health insurance premium in the Netherlands is about EUR 1,900 (USD 2,162).21 Premiums have risen significantly from the average of EUR 1,400 (USD 1,593) in 2020, outpacing the rate of inflation and the rise in the health care allowance for people on lower incomes (see Safety Nets). In addition, everyone pays 9.7 percent of their income — up to an annual ceiling of EUR 38,441 (USD 43,736) — to fund the long-term care system.22
As of 2025, employer contributions are levied at 6.5 percent of a person’s income, up to a maximum annual income ceiling of EUR 75,864 (USD 87,230).23 The contribution rate for self-employed individuals is 5.3 percent.24 All contributions are pooled in a central health insurance fund that’s supplemented by central government tax revenue. Funds are then distributed to health insurers (based on employee health risk profiles) and municipal funds and used to cover the costs associated with the health care allowance and health care for those under age 18.25
Some treatments, such as general physiotherapy, are only partially covered (that is, they are only covered for people with specific chronic conditions). Some elective procedures are excluded, such as dental care after age 18 and eye care without medical indication. Medical devices are covered under statutory basic health care insurance if they are suitable and not unnecessarily expensive. Medical devices and aids may require permission from the health insurer.27
The Netherlands provides subsidies (health care allowances) to help cover the cost of insurance premiums for lower-income individuals. As of 2025, eligible single people must have an annual income of less than EUR 39,719 (USD 45,660), and households must have an annual income of less than EUR 50,206 (USD 57,720).28 The allowances are means-tested up to a maximum of EUR 131 (USD 150) per month for single people and EUR 250 (USD 287) per month for households.29
The government also provides safety nets for uninsured individuals through two government programs:30
The regulation for uninsured foreign individuals covers uninsured non-E.U. migrants without a residence permit, including asylum seekers awaiting status decisions. It reimburses both care under the Zvw and the Wlz.
The subsidy program for medically necessary care for the uninsured applies to uninsured E.U. residents, including homeless individuals and former migrant workers, and covers only basic health care under the Zvw.
In 2023, total spending under the SOV increased from EUR 44.5 million (USD 52 million) in 2021 to EUR 74 million (USD 86 million). This increase has been attributed to inflation, increased awareness of the program, and the larger number of uninsured individuals requiring care. Despite this growing need, the government has proposed reducing the program’s budget by more than half from 2027 and limiting its coverage to acute care only.31
There are no separate safety nets for prescription medicines, as the basic health care insurance already covers the majority of them (see Services Covered by Public Health Insurance).
The Role of Private Health Insurance
In 2025, 80.6 percent of individuals with statutory basic health care insurance purchased some form of supplementary private insurance.32 Most plans are complementary, in that they provide coverage for services excluded from, or not fully covered by, the statutory basic health care insurance. Such services include dental care, physiotherapy, eye care, contraceptives, medical care abroad, and alternative medicine. The plans also reduce copayments or cover them entirely. Depending on the specific package, supplementary insurance may provide access to a broader network of providers and faster specialist appointments than are available under statutory basic health care insurance.33
Most individuals who purchase voluntary insurance do so from the same insurer that provides their statutory cover. In most cases, children are covered for the services included in a supplementary plan taken out by their parents.34
The Role of Government
Since the implementation of the Zvw, the role of the government in health care has primarily been to regulate the system from a distance, rather than managing it directly.35 The Ministry of Public Health, Welfare and Sport has oversight of health care policies and priorities. It is responsible for setting the standard benefits package and annual health care budget; introducing legislative changes when necessary; and monitoring access, quality, and costs across the market-based system.36
Following a number of decentralizing reforms in 2015, municipal authorities have shared an increasing share of the VWS’s duties. In addition, disease prevention and health promotion are largely the municipalities’ responsibility.37
A number of independent agencies are responsible for setting operational priorities and acting in a supervisory and advisory capacity, as part of the multistakeholder decision-making framework:
At the national level, the Health Council of the Netherlands (Gezondheidsraad) advises the government on evidence-based medicine, health care, public health, and environmental protection.38
The Medicines Evaluation Board (College ter Beoordeling van Geneesmiddelen) oversees the efficacy, safety, and quality of medicines.39
The National Health Care Institute regularly reviews existing benefits and advises the government on what should be included in the mandatory benefit package, focusing on proven and appropriate care.40
The Dutch Health Care Authority (Nederlandse Zorgautoriteit [Nza]) regulates and supervises important aspects of the health insurance system, including care contracting and provider pricing, to promote accessible and affordable care.41
The Health and Youth Care Inspectorate (Inspectie Gezondheidszorg en Jeugd [IGJ])supervises the quality, safety, and accessibility of care. Self-regulation by physicians is an important aspect of the system.42
Integration and Care Coordination
Since the 2000s, the areas of financing, elderly care, and general practitioner (GP) payments have seen reforms aimed at strengthening the cooperation between primary and community care services.43 These reforms include a bundled payment system for managing chronic conditions, such as type 2 diabetes, seeking to align provider incentives and reduce fragmentation in care delivery.44
GPs are responsible for the initial coordination of care for common chronic conditions and mental health services and for referrals to most secondary care.45 Private health insurers can compete with each other by offering more attractive and integrated care arrangements across statutory and complementary (voluntary) health insurance plans.46
Operations and Resources
Overview of the Delivery System
The health care system can be categorized into two groups:47
Primary care includes general practice, screening and prevention programs, oral health, pharmacies, some mental health care, and primary eye care services.
Secondary care includes the planned or elective care usually provided in hospitals, urgent and emergency care (including telephone services), ambulance services, after-hours GP services, and mental health care.
The payment system for GPs is based on a three-segment model that was introduced in 2015:48
Segment 1 (about 75 to 80% of GP income) covers core primary care services and consists of a capitation fee for each registered patient, consultation fees (phone or home visits), and fees for ambulatory mental health care at the GP practice.
Segment 2 (about 15% of GP income) reimburses multidisciplinary care for chronic conditions. This segment operates through a system of bundled payments negotiated between insurers and GP-owned care groups.
Segment 3 (5 to 10% of GP income) gives GPs and insurers the opportunity to negotiate additional contracts that encourage innovation and tie payment to performance.
The payment mechanism for hospitals and medical specialists is based on a diagnosis-treatment combination system that assigns a price to a bundle of activities required to treat specific diagnoses. Most DBC prices are negotiable between insurers and hospitals, and the Dutch Health Care Authority sets the maximum prices for complex treatments. Since 2015, specialists’ remuneration has been integrated into DBC prices, and hospitals negotiate with medical specialist firms about their pay.49
Primary Care
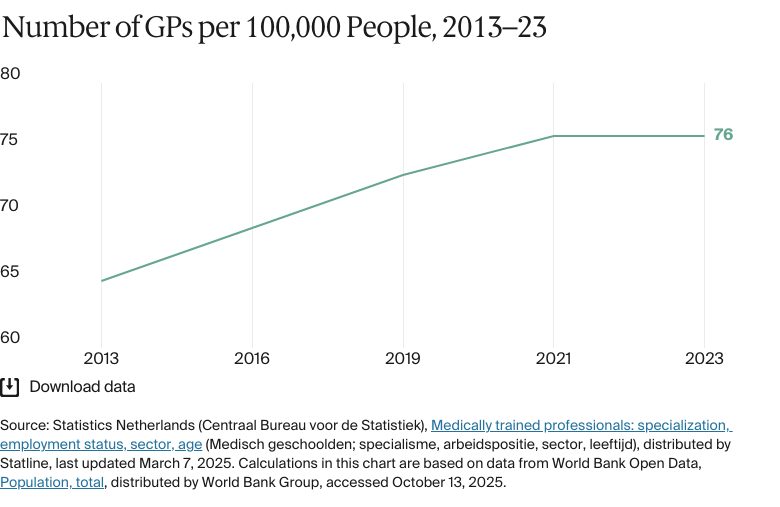
In 2023, there were 372 doctors for every 100,000 people.50 In the same year, there were 13,595 registered GPs — 76 for every 100,000 people.51
Primary health care is delivered by a range of private providers, including GPs, practice nurses, dentists, midwives, physiotherapists, and psychologists.52 GPs are most patients’ first point of contact and act as official gatekeepers, with referrals required for most secondary care services.53 Over the past decade, responsibility for some tasks has shifted from GPs to other professionals, such as practice nurses and therapists.54
Most GPs work independently, but the number of independent GPs has been declining (from 87% of practitioners in 2012 to 64% in 2023) as more come to work in salaried positions or as permanent locums.55 GPs are also more likely to work in group or duo practices (with two regular GPs); only 7 percent were working in solo practices in 2022.56
Registration with a GP is not mandatory, but most citizens (95%) are registered with one in their local area. GPs can refuse to take on patients, and numbers per practice are limited, so patient choice might be restricted (60% of GP practices stopped accepting new patients in 2024).57
As of January 2024, there were 4,837 GP practices, of which 84 percent were dual or group practices, and 16 percent operated with a single GP.58 The past decade has seen a trend of consolidation toward larger group practices, alongside a growing emphasis on multidisciplinary care teams where GPs collaborate with other professionals such as physiotherapists, midwives, and mental health specialists.59 Many GP practices offer broad service profiles, including specialist nurses.60
Chronic care management is coordinated through care groups, which are mostly GP networks. Care groups are legal entities that assume clinical and financial responsibility for enrolled chronic disease patients and purchase services from multiple providers.61
Out-of-hours care is organized at the municipal level in “GP posts.” These are walk-in centers, typically run by a nearby hospital, that have a gatekeeping function for emergency care. Nearly every GP works for a GP post through a cooperative, receiving an hourly compensation rate.62
Outpatient/Specialist Care
Secondary care typically involves specialized medical attention that patients access through a GP referral. Most specialists work out of hospitals and mental health care centers rather than in private clinics. There are specialist clinics for certain services, such as sexual health and acute mental care, which also require a GP referral. Without a referral, patients need to use private insurance or pay out of pocket.63
Over the past decade, the rising complexity of health care needs has led to a gradual shift toward increased clinic specialization within hospitals. Once patients receive a referral for specialist treatment (in any hospital), they are free to choose their provider. Insurers may set various conditions, such as cost sharing, that apply when choosing particular specialists.64
In 2023, there were 23,720 medical specialists, equivalent to 133 for every 100,000 people.65 The majority of these specialists are hospital-based (mostly in general and university hospitals) and are either part of a group practice or salaried.66
Physician Education and the Workforce
In 2024, about 1.7 million people, or over 17 percent of the working-age population, were employed in the health care sector.67 Foreign-trained health care workers made up 3.6 percent of doctors and 1.4 percent of nurses in 2023. There’s no significant trend of health care professionals leaving the country to work abroad.68
The health care sector struggles with workforce retention, often because of dissatisfaction over pay, the working environment, career growth, and workloads. Many medical professionals choose to freelance because of the greater flexibility doing so offers; this can contribute to inefficiencies and scheduling challenges for permanent staff.69
There’s the very practical problem of health workforce shortages, mostly in rural or periphery areas near the borders, which is especially apparent in primary care.
Luc Hagenaars
Assistant Professor of Health Policy Analysis
Amsterdam University Medical Centre (UMC)
In a 2023 report, the Council for Public Health & Society, an independent advisory body to the government, said that the Dutch health care system was likely to face a growing shortage of GPs over the coming years, with scarcity issues also arising among certain specialist roles, including psychiatry, pediatrics, addiction medicine, and geriatrics.70
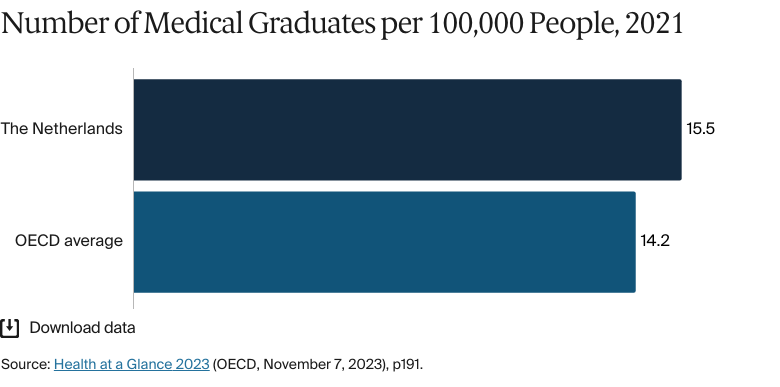
In 2021, there was an average of 15.5 medical graduates for every 100,000 people, close to the E.U. average.71 By 2023, the number had dropped to 14 medical graduates for every 10,000 people. The number of medical doctors is regulated through caps on medical students at both the national and university level. In 2022, the government recommended the provision of 6,438 intake places for medical, dental, and mental health courses; 59 percent of these spaces were for medical training.72
As of the 2025–26 academic year, medical students pay a yearly tuition fee of EUR 2,601 (USD 3,059).73 The fee is higher for non–European Economic Area students — between EUR 20,900 and EUR 32,000 a year (USD 24,583 and 37,640).74 To match supply to demand, a capacity assessment body advises the Ministry of Health, Welfare and Sport on all specialized postgraduate training programs for medical specialists.75
Hospitals
Nearly every hospital is a private nonprofit institution. In 2025, 69 hospital organizations operated a total of 113 hospitals and 137 outpatient clinics.76
There are three main types of hospitals, the majority being general hospitals, which are located around the country. In addition, there are eight academic hospitals affiliated with major universities. Each has a research focus, serves as a teaching hospital, and offers specialized services such as neurosurgery and advanced oncology, infectious disease care, and most of the country’s high-level pediatric care. There are also a number of specialized hospitals, such as the Netherlands Cancer Institute in Amsterdam and the national Major Incident Hospital located in UMC Utrecht. These also serve as teaching hospitals.77
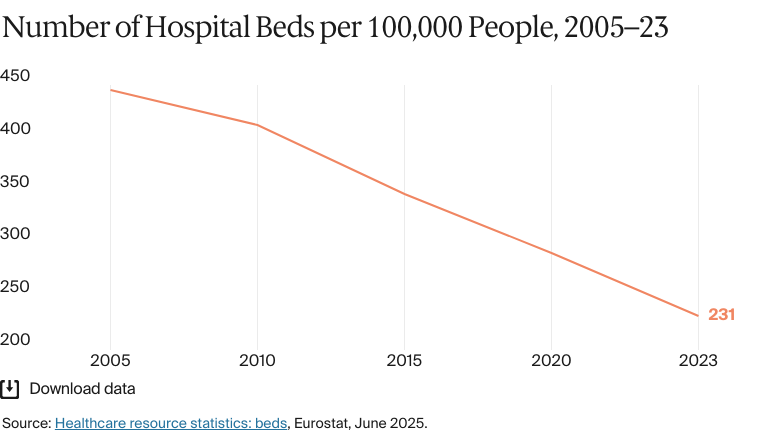
In 2023, there were 231 hospital beds for every 100,000 people, less than half the E.U. average of 511.78 This low bed capacity is a reflection of strict gatekeeping at primary care level, a high rate of day surgeries, and the accessibility and effectiveness of outpatient (and home care) services.79
The Netherlands has one of Europe’s higher ratios of nursing and midwifery professionals: 1,167 for every 100,000 people in 2022.80 This compares with 770 across the E.U. Nursing shortages in hospitals are an issue, however, and the nursing workforce is overstretched, partly because of outflows during the COVID-19 pandemic.81 Several reforms over the past decade have given nurses the right to take over more advanced tasks from GPs and to prescribe certain medications.82
Mental Health Care
BY THE NUMBERS
In 2023, the Netherlands had more than 25 psychiatrists per 100,000 inhabitants (among the highest ratios in the E.U.).83
In 2023, there were 206 mental health care professionals per 100,000 people.84
Mental health care is well integrated into the health system. Overseen by the government, the Dutch Association of Mental Health and Addiction Care (Geestelijke Gezondheidszorg [GGZ] Nederland) delivers services through a network of mental health care facilities and professionals.85
The first point of contact for mental health care is the GP, who refers the patient to primary or secondary mental health care services based on the severity of the condition.86 Primary care, typically managed by GPs and practice nurses, addresses mild mental health issues and can provide referrals to psychologists or psychotherapists for more complex cases. Secondary care, including treatment for conditions such as depression or post-traumatic stress disorder, is typically managed by multidisciplinary teams in mental health institutions.87
Outpatient mental health care is covered as part of the statutory basic health care insurance.88 Inpatient care might be covered, subject to the mandatory deductible and the type of condition.89 Cost-sharing arrangements for people with more severe, longer-term mental health disorders are regulated under the Wlz (see Long-Term Care and Social Support).90 Hospitals provide acute mental health care.91In 2023, there were 15,916 beds available through the country’s mental health care system.92
As in many countries, mental health issues are on the rise. The prevalence of disorders in the Netherlands is higher than the average for high-income countries (see Health Outcomes). Wait times have grown longer, particularly for specialist care. In 2022, about two-thirds of patients referred to specialist mental health services waited more than four weeks for an initial consultation, with 30 percent waiting more than 10 weeks for treatment.93 About 78,000 people were on the wait list for mental health services at the end of 2023. The reasons for this include limited care capacity and a shortage of mental health professionals, especially in child services, where delays tend to be longer.94
Issues with financing incentives have also been problematic, Hagenaars says. “It has tended to be more lucrative for health insurers to cover and for providers to provide low-intensity mental health care, leaving less resources available to those in need of more severe mental health care,” he notes. “And that’s obviously problematic, [in that it leads] to long wait lists for those in more urgent need of care.”
Since 2021, the government has introduced several initiatives aimed at improving access to mental health care and reducing wait times. These include a revised remuneration system for mental health providers to address skewed incentives, and a new coordination mechanism among health care providers, GPs, municipalities, and insurers that enables them to transfer patients to a service provision with treatment capacity.95
Long-Term Care and Social Support
The Netherlands’ universal coverage of long-term care is comprehensive in its scope.96 Based on the Wlz, long-term care operates through a statutory social insurance system that is financed primarily through income-related premiums, taxes, and income-related copayments (as of 2023, this is 9.7% of individual income, up to an annual income threshold).97
Wlz covers institutional, residential, and home-based care for patients in need of permanent supervision and for people with severe mental or physical disabilities.98 The Care Needs Assessment Centre, a governmental agency, determines eligibility based entirely on clinical need.99 In 2022, 400,975 individuals used Wlz care services.100
Most other home-based nursing and personal care is covered by statutory basic health care insurance alongside municipal-level funding for community-led social care services regulated under the Wmo.101
These laws are intended to improve the quality of care and to keep health care available and affordable. While chronically ill people are initially encouraged to seek help within their own network, an aging population and the high number of people suffering from chronic illnesses make this unfeasible.102 Long-term care comes at a public cost: government spending (as a share of both gross domestic product [GDP] and total health expenditure) is among the highest within the Organisation for Economic Co-operation and Development (OECD).103 “A significant portion of health care spending goes to long-term care, which is unusual given that the country is not as aged as some others like Germany,” Hagenaars says.
Since 2015, some long-term care responsibilities have been transferred to municipalities, most notably under the Wmo. These responsibilities include support for independent living at home for frail older people and the provision of social long-term care services.104 Municipalities provide this support directly or with assistance from health care providers.105 Municipal authorities receive a non-earmarked budget from the central government to fund these services rather than relying on their own tax-raising capacity.106
Cost sharing depends on annual income and wealth, the age of the insured, and household size. For residential long-term care, there’s an income- and wealth-related copayment of up to a maximum of EUR 2,954 (USD 3,360) per month.107
Cost and Affordability
Health Care Spending Overview
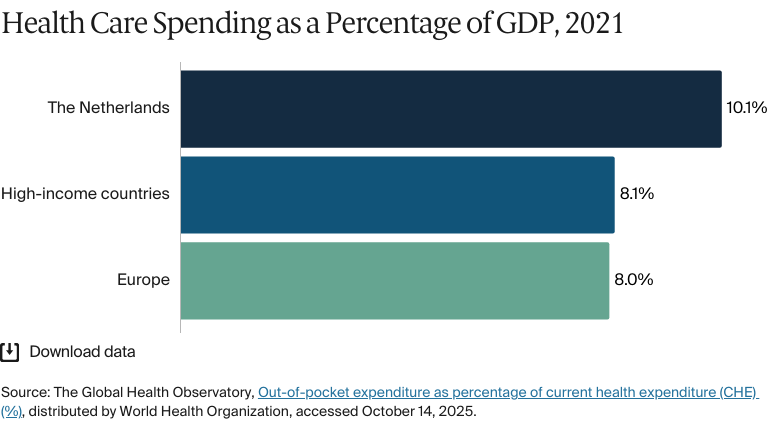
In 2022, 10.1 percent of the Netherlands’ GDP was spent on health care — above the average for high-income countries (8%).108 The ratio has been fairly stable over the past decade, but it rose to 11.1 percent in 2020–21 because of increased spending during the COVID-19 pandemic.
Health expenditure per capita totaled EUR 5,470 (USD 5,796) in 2022, well above the E.U. average of EUR 3,685 (USD 3,880).109In 2024, government spending and compulsory statutory health care insurance funded most of that health expenditure (83.2%), followed by out-of-pocket spending (11.8%) and voluntary private payments (5%).110
The share of out-of-pocket spending is about two-thirds of the average level in the E.U.111 Voluntary private payments mainly go toward supplementary health insurance contributions to cover services outside of statutory basic health care insurance.112
In 2023, the largest share of total health expenditure was allocated to long-term care (29.1%), followed by outpatient care (27%) and inpatient care (22%).113
Pharmaceutical Spending
Expenditure per capita on prescription and over-the-counter medicines was EUR 436 (USD 507) in 2024, among the lowest of all OECD countries.114 Pharmaceutical spending made up 7 percent of all health care spending in 2022 — the second lowest share among OECD countries.115
This low level of pharmaceutical spending is a result of:116
Comparatively tight pricing and reimbursement regulations
Extensive cross-sector agreements between health insurers, health care providers, and patient organizations on drug prices and usage
The widespread use of generic medicines.
Most prescription medicines are reimbursable (either fully or through cost sharing) under statutory basic health care insurance.117 Most insurers have a “preferred medicine policy,” under which they select one brand from a group of products with the same active ingredients (usually the cheapest available generic option) to reimburse.118
Cost Sharing and Out-of-Pocket Spending
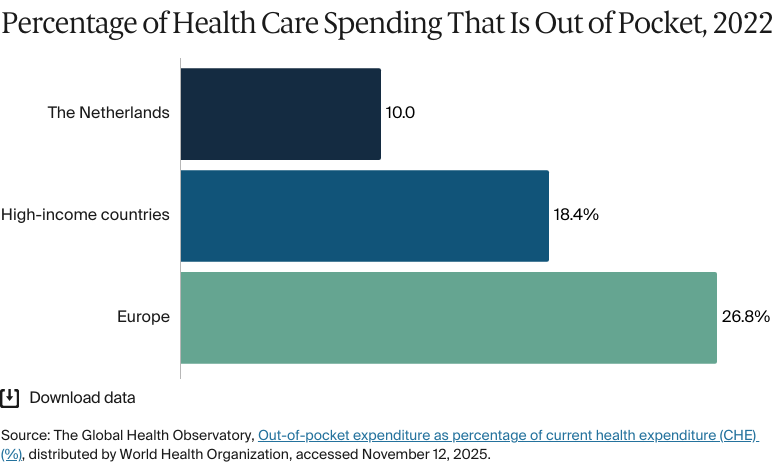
Out-of-pocket spending made up 10 percent of total health expenditure in the Netherlands in 2022, below the European average of 26.8 percent and the high-income country average of 18.4 percent.119
In 2021, the largest share of out-of-pocket spending was on pharmaceuticals (21%), followed by inpatient care (19%) and long-term care services (17%).120
As of April 2025, the main form of cost sharing in the statutory health care insurance system is a compulsory annual deductible of EUR 385 (USD 438).121 All adults over age 18 are required to pay up to this level before the insurer begins to cover most health care services under the standard benefits package, which include hospital treatment, diagnostic tests, specialist care, and prescription drugs.122
Citing concerns about unequal access to care, the country’s four-party coalition government (which has been in office since mid-2024) has set out plans to lower the deductible to EUR 165 (USD 188) from 2027. It will also introduce a maximum deductible payment of EUR 50 (USD 57) per hospital treatment.123
Policyholders have the option to pay an additional voluntary deductible, up to a maximum of EUR 500 (USD 569), in exchange for lower monthly insurance premiums. In 2024, most enrollees (85%) chose not to pay any additional deductible, but about 10 percent paid the maximum.124 The deductible doesn’t apply to GP visits, obstetric and maternity care, community nursing, care for certain chronic diseases, or care for children up to age 18, all of which are provided free of charge.125
Since 2019, patient copayments for prescription drugs have been capped annually at EUR 250.126 The most common direct payments for health services not covered by basic health care insurance are for dental care, adult physiotherapy, and long-term care. Income-dependent cost sharing also applies to residential long-term care.127
How Are Costs Contained?
Pharmaceutical cost containment has been a focus of successive governments, particularly as newer, more expensive treatments are developed. Pricing for prescription drugs is regulated by the Medicines Prices Act 1996, under which the state fixes a maximum wholesale price for all authorized medicinal products based on the average cost of comparable products in four reference markets (currently Belgium, France, Norway, and the U.K.).128
Within the WGP framework, health insurers, pharmacists, and hospitals often enter into contractual arrangements around specific drug prices, generic substitutions, and economies of scale. Additionally, many insurers adopt a preferential policy that covers only the cheapest generic version of a medicine containing the same active ingredient as the branded drug.129
The WGP also incorporates a “lock” procedure that withholds new innovative medicines from general use until the National Health Care Institute has examined their effectiveness relative to price.130 There are two thresholds for the lock: 1) where the product cost would be more than EUR 20 million (USD 23 million) a year for one or more treatments or 2) where costs per patient would be more than EUR 50,000 (USD 56,888) a year and the annual cost would exceed EUR 10 million (USD 11 million).131
A study commissioned by the National Health Care Institute in 2023 declared that the lock system had delivered significant cost savings over the past decade. However, the study also acknowledged its potential to limit returns on investment for pharmaceutical companies and to restrict the availability of medicines for rare diseases.132
Another significant step is the modernization and regular review of the Medicines Reimbursement System. This system determines which medicines are reimbursed by health insurers and sets a maximum reimbursement for each group of drugs. If a medicine exceeds this, patients must cover the difference.133
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
Average life expectancy at birth was 81.9 years in 2024.134
The avoidable mortality rate was 149 per 100,000 people in 2023.135
Mental disorders and diseases of the nervous system: 132 per 100,000 people.
The maternal mortality rate was 4.3 deaths per 100,000 live births in 2023 (compared with 11 on average in Europe).137
The infant mortality rate was 3.6 deaths per 1,000 live births in 2023 (compared with four on average in high-income countries).138
The share of the population with mental health disorders was 18 percent in 2021 (compared with 16% on average in high-income countries).139
The suicide rate was 12.3 per 100,000 people in 2023 (compared with an average of 12 in high-income countries).140
Guns are responsible for 0.42 deaths in every 100,000 in the Netherlands.141
15 percent of adults were affected by obesity in 2022.142
In 2024, average life expectancy was 81.9 years, slightly higher than the average for countries in the E.U. (80.9 years). There was a three-year difference between the life expectancies of men (80.5 years) and women (83.3 years) — a narrower gap than in many E.U. countries.143
Mortality rates for preventable and treatable causes are lower than in many other high-income countries and trended downward in the decade prior to 2019. COVID-19 deaths (classified as preventable) lifted the avoidable mortality rate in 2020–21, as they did elsewhere, but in 2022, the rate returned close to the pre-pandemic level.144
Noncommunicable diseases typically account for more than 90 percent of deaths. Apart from COVID-19, the leading causes of death are cardiovascular disease, cancer, and dementia.145
The suicide rate has remained stable over the past decade. On average, men are two and a half times more likely than women to take their own lives. In the past decade, rates have been highest for people ages 40 to 59.146
Addressing Health Inequities
The share of the population reporting an unmet need for medical care due to cost was 0.3 percent in 2023, among the lowest rates in the E.U.147
State-backed compensation (and, in some cases, exemptions) are available for low-income groups and unemployed people to help with the cost of the mandatory deductible and basic health care insurance premiums. However, pressure on household finances has seen more people avoid care due to financial concerns. The planned reduction in the mandatory deductible from 2027 aims to address this (see Cost Sharing and Out-of-Pocket Spending).148
In 2018, the government established the National Prevention Agreement with 70 social partners, which set a range of nonbinding targets and recommended measures to reduce smoking, obesity, and problematic alcohol consumption by 2040. A 2024 review by the National Institute for Public Health and the Environment found that, while there had been some progress, especially in terms of reducing overall smoking prevalence, it was unlikely that the 2040 targets would be achieved.149
Non-European migrants are at higher risk for mental health problems and communicable and noncommunicable diseases than ethnic Dutch residents; they also have a higher mortality rate.150 Language barriers contribute to this discrepancy, with the availability of translators being limited by budget cuts. Additionally, some services are available only by phone, leading to privacy concerns.151 Migrants have also reported discrimination, with studies finding that migrants did not trust health care workers to take their problems seriously.152
Innovation and Reform
Health Care Innovation
In 2022–23, the health system implemented a new cross-sectoral Integrated Care Agreement strategy. Comprising about 400 separate agreements, it aims to strengthen cooperation between health care providers at the regional level and between GP practices and mental health providers. It also seeks to improve basic community care, health prevention, insurer–provider contracts, and the digitalization of patient data.153
In 2022, the government introduced a five-year, multistakeholder agreement to help older people remain at home as long as possible by keeping fit and using assistive devices. Known as Housing, Support and Care for Older People, the agreement includes incentives to subsidize housing initiatives and at-home adaptations. The Dutch Health Care Authority, however, states that many projects hadn’t been fully implemented as of 2024.154
Reforms to GP reimbursement in 2018 aimed to improve compensation mechanisms for complex consultations, expand support for chronic illness and elderly care, and encourage innovations in digital and out-of-hours services.155 Since 2022, a new fee-for-service performance payment model for adult mental health care has been in place to contain costs and simplify financing.156
Other recent regulatory changes include the Healthcare Providers Admission Act 2022, which is aimed at strengthening regulations and fraud prevention in the licensing of health care providers, and revisions in 2023 to the WPG to strengthen legal provisions relating to collective measures during pandemics.157
Health Care Technology
All GPs use an electronic information system to record patient medical data, which are integrated into an electronic prescription system. Since 2020, patients have had the legal right to access their digital health records independently through a patient portal or secure online platforms known as personal health environments (PBLs). Patients can get data from multiple health care settings, including hospitals and pharmacies, offering them a means to track treatment plan details, laboratory results, and medical prescriptions. While the GP portals are well integrated, the interoperability of PBLs can be limited.158
In April 2025, a range of insurers and health care providers signed an agreement with the government to strengthen the sharing of electronic information on bed and care capacity across health care settings, including emergency, primary, acute, maternal, and mental health care.159
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Roland Bertens and Jasmin Palamar, Dutch Healthcare Policy in Historical Perspective, 1941–2017 (Het Nederlandse zorgbeleid in historisch perspectief, 1941–2017) (Scientific Council for Government Policy [Wetenschappelijke Raad voor het Regeringsbeleid], September 14, 2021), https://www.wrr.nl/publicaties/working-papers/2021/09/14/nederlandse-zorgbeleid-in-historische-perspectief. This paper gives a summary of Dutch public health care policy, starting with the Health Insurance Decree 1941.
↩
Ministry of Public Health, Welfare and Sport, Healthcare in the Netherlands.
↩
8
Ministry of Public Health, Welfare and Sport, Healthcare in the Netherlands.
↩
9
Ministry of Public Health, Welfare and Sport, Healthcare in the Netherlands.
↩
10
Hans Maarse et al., “Organization and financing of public health services in Europe: country reports,” in Health Policy Series 49, edited by B. Rechel et al. (European Observatory on Health Systems and Policies, 2021), https://www.ncbi.nlm.nih.gov/books/NBK507329/.
↩
“Key figures for health insurers” (Kerncijfers zorgverzekeraars), Dutch Healthcare Authority (Nederlandse Zorgautoriteit), accessed October 26, 2025, https://www.nza.nl/zorgsectoren/zorgverzekeraars/kerncijfers-zorgverzekeraars. This statistical summary offers various health insurance figures for 2025, including the number of health insurers and percentage of insured persons.
↩
Ministerie van Volksgezondheid, Welzijn en Sport (Netherlands), “Regeling geraamde gemiddelde nominale premie 2025 (BWBR0050321),” Wetten.nl, issued October 14, 2024, version effective January 1, 2025, accessed February 19, 2026, https://wetten.overheid.nl/BWBR0050321/2025-01-01. Article summarizing the rise in health premiums in the Netherlands between 2020 and 2025.
↩
Ministry of Public Health, Welfare and Sport, Healthcare in the Netherlands.↩
26
“Zvw compass: reimbursements from the basic package” (Zvw-kompas: vergoedingen uit het basispakket), Dutch Healthcare Institute (Zorginstituut Nederland), accessed October 26, 2025, https://www.zorginstituutnederland.nl/Verzekerde+zorg/zvw-kompas. An overview of how reimbursements are arranged under basic health care insurance.
↩
“Nza role and duties: what the Dutch Healthcare Authority (Nza) does in brief,” Dutch Healthcare Authority, accessed October 26, 2025, https://puc.overheid.nl/nza/doc/PUC_276485_22/1/ (accessed July 25, 2025).
↩
“Declarations and rates” (Declareren en tarieven), Landelijke Huisartsen Vereniging, accessed October 26, 2025, https://www.lhv.nl/thema/praktijkzaken/declareren-en-tarieven/. “How does billing for your care work, what are the rates, and how is GP care funded?”.
↩
Statistics Netherlands, Medically trained professionals; World Bank Open Data, Population, total, distributed by World Bank Group, accessed October 10, 2025, https://data.worldbank.org/indicator/SP.POP.TOTL?locations=DE-NO-NL. In-text statistics calculated using these population figures; The Global Health Observatory, Medical doctors (per 10,000).
↩
51
Statistics Netherlands, Medically trained professionals; World Bank Open Data, Population, total; The Global Health Observatory, Medical doctor: generalist medical practitioners (number), distributed by World Health Organization, accessed April 21, 2025, https://www.who.int/data/gho/data/indicators/indicator-details/GHO/generalist-medical-practitioners-(number); World Bank Open Data, Population, total. In-text statistics calculated using these population figures.
↩
Henriëtte E van der Horst and Niek de Wit, “Redefining the core values and tasks of GPs in the Netherlands (Woudschoten 2019),” British Journal of General Practice 70, no. 690 (2020):38–39, https://doi.org/10.3399/bjgp20X707681; Karin Hek and Joost Vanhommerig, “Annual figures for general practitioner care 2024: the number of consultations with the POH-GGZ continues to increase” (Jaarcijfers huisartsenzorg 2024: het aantal consulten bij de POH-GGZ blijft toenemen), Nivel, June 17, 2025, https://www.nivel.nl/nl/nieuws/jaarcijfers-huisartsenzorg-2024-het-aantal-consulten-bij-de-poh-ggz-blijft-toenemen. Analysis of the increase in demands on GP mental health services in 2024; “Doubling of the number of practice assistants in primary care since 2016” (Verdubbeling aantal praktijkondersteuners in de huisartsenzorg sinds 2016), ZorgKrant.nl, last updated September 11, 2023, https://zorgkrant.nl/acute-zorg/17610-verdubbeling-aantal-praktijkondersteuners-in-de-huisartsenzorg-sinds-2016. Overview of the increase in GP practice assistants.
↩
55
Nivel, Primary care: services: general practitioners, distributed by VZinfo, 2023, https://www.vzinfo.nl/eerstelijnszorg/aanbod/huisartsen; L.E. Flinterman et al., General Practitioners and Practices in the Picture: Figures from Nivel Professional Registrations in Healthcare 2023–2024 (Huisartsen en praktijken in kaart: Cijfers uit Nivel beroepenregistraties in de zorg 2023–2024) (Nivel, 2025), https://www.nivel.nl/sites/default/files/bestanden/1004735_0.pdf. This report covers the development of GP numbers and practices in the Netherlands up to 2023–2024.
↩
European Observatory on Health Systems and Policies, “Netherlands.”
↩
65
Statistics Netherlands, Medically trained professionals; World Bank Open Data, Population, total. In-text statistics calculated using these population figures.
↩
“Healthcare and welfare labor market” (Arbeidsmarkt zorg en welzijn), Central Agency for Statistics (Centraal Bureau voor de Statistiek), https://www.cbs.nl/nl-nl/dossier/arbeidsmarkt-zorg-en-welzijn. Overview of demand for and shortage of healthcare professionals in the Netherlands.
↩
68
Varkevisser et al., Sustainability and Resilience.↩
69
Laura Elizabeth Verhage, “Retention and Recruitment of Healthcare Professionals in the Netherlands: Prospects for Central Government Steering Strategies” (Bachelor’s thesis, Tilburg Law School, 2022), https://arno.uvt.nl/show.cgi?fid=172099.
↩
70
Getting the Basics Right: Principles for Future-Oriented Primary Care (De basis op orde: Uitgangspunten voor toekomstgerichte eerstelijnszorg) (Council for Public Health and Society [Raad Volksgezondheid & Samenleving], April 3, 2023), https://www.raadrvs.nl/documenten/publicaties/2023/04/04/de-basis-op-orde. An RVS report on the need for a reorganization of primary care.
↩
Capacity Assessment Body (Capaciteitsorgaan), “Education: recommended entry-level medical, dental and mental health care” (Opleidingen: geadviseerde instroom geneeskundig, tandheelkundig en GGZ), State of Public Health and Care (De Staat van Volksgezondheid en Zorg), 2022, https://www.staatvenz.nl/kerncijfers/opleidingen-geadviseerde-instroom-geneeskundig-tandheelkundig-en-ggz. Figures on the recommended number of entry places for medical training.
↩
National Institute for Public Health and the Environment (Rijksinstituut voor Volksgezondheid en Milieu), Hospital care: services: institutions, distributed by VZinfo, last updated May 21, 2025, https://www.vzinfo.nl/ziekenhuiszorg/aanbod/instellingen.
↩
77
National Institute for Public Health and the Environment, Hospital care; “Hospital care: general and academic hospitals” (Ziekenhuiszorg: Algemene en academische ziekenhuizen), Atlas van Zorg & Hulp, accessed October 26, 2025, https://zorghulpatlas.nl/zorg-in-nederland/ziekenhuiszorg/algemene-en-academische-ziekenhuizen/?utm . “What is the difference between general and academic hospitals?”; “How is healthcare organized in the Netherlands?” (Hoe is de zorg in Nederland geregeld?), National Contact Point for Cross-Border Care (Nationaal Contactpunt voor Grenoverschrijdende zorg), last updated March 13, 2023, https://cbhc.hetcak.nl/nl/behandeling-in-nederland/zorg-nederland-geregeld-0/?utm. A basic guide to health care in the Netherlands for non-citizens.
↩
“Mental health care: medically trained” (GGZ: Medisch geschoolden), State of Public Health and Care (De Staat van Volksgezondheid en Zorg), 2023, https://www.staatvenz.nl/kernScijfers/ggz-medisch-geschoolden. Figures on the number of medically trained people working in mental health care in the Netherlands; World Bank Open Data, Population, total. In-text statistics calculated using these population figures.
↩
“Psychological help provided by a general practitioner or other healthcare providers within mental health care” (Psychische hulp door huisarts of andere zorgaanbieders binnen ggz), Government of the Netherlands, accessed 26 October 2025, https://www.rijksoverheid.nl/onderwerpen/geestelijke-gezondheidszorg/psychische-hulp-huisarts-of-ggz. An overview of GP-provided mental health care in the Netherlands.
↩
87
Government of the Netherlands, “Psychological help”; Kroneman et al., Netherlands Country Health Profile.
↩
88
Government of the Netherlands, “What care is included.”
↩
Kroneman et al., Netherlands Country Health Profile.
↩
94
Bas de Vries, “Patients and healthcare providers challenge the state and insurers to reduce long waiting lists for mental health care” (Patiënten en zorgverleners dagen Staat en verzekeraars om lange wachtlijsten ggz), Nos News (NOS Nieuws), May 30, 2024, https://nos.nl/artikel/2522419-patienten-en-zorgverleners-dagen-staat-en-verzekeraars-om-lange-wachtlijsten-ggz. News article on a case brought against insurers for not purchasing enough mental health care; Kroneman et al., Health System Summary.↩
95
Kroneman et al., Netherlands Country Health Profile.
↩
96
Pieter Bakx et al., “Long-term care in the Netherlands,” Working Paper No. w31823, National Bureau of Economic Research, November 2023, https://www.nber.org/papers/w31823.
↩
97
Yeeun Lee and David Knapp, Netherlands 24-Hour Long-Term Care Benefits Plan Details 2015–2024, (University of Southern California, 2024), https://g2aging.org/ltc/api/download/pdf/3/14.
↩
Varkevisser et al., Sustainability and Resilience.↩
119
The Global Health Observatory, Out-of-pocket expenditure.
↩
120
Kroneman et al., Netherlands Country Health Profile.
↩
121
“Care” (Zorg), Government of the Netherlands (Rijksoverheid), accessed October 26, 2025, https://www.rijksoverheid.nl/regering/regeerprogramma/6a-zorg. Government publication on planned amendments to improve health care in the Netherlands.
↩
Institute for Health Metrics and Evaluation, GBD Compare, distributed by IHME, 2023, https://vizhub.healthdata.org/gbd-compare/. Overall firearm mortality is an aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
Alina Ioana Forray et al., “Uncovering multi-level mental healthcare barriers for migrants: a qualitative analysis across China, Germany, Netherlands, Romania, and South Africa,” BMC Public Health 24 (2024):1593, https://doi.org/10.1186/s12889-024-19046-z; Abdulhakeem Al-Tamimi et al., “Yemeni refugees’ health literacy and experience with the Dutch healthcare system: a qualitative study,” BMC Public Health 23 (2023):902, https://doi.org/10.1186/s12889-023-15732-6.↩
“The integrated care agreement: working together for healthy care” (Het Integraal Zorgakkoord: samenwerken aan gezonde zorg), Government of the Netherlands (Rijksoverheid), accessed October 26, 2025, https://www.rijksoverheid.nl/onderwerpen/kwaliteit-van-de-zorg/integraal-zorgakkoord. An overview of the integrated care agreement between the government and health care professionals.
↩
“More insight into online access” (Meer inzicht in online inzage), Dutch College of General Practitioners (Nederlands Huisartsen Genootschap), April 17, 2024, https://www.nhg.org/thema/digitale-zorg/online-inzage/online-inzage-medisch-patientendossier. An article announcing the publication of the “Practical Guide to Online Access,” containing “concrete practical advice and practical tools for policy decisions”.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.