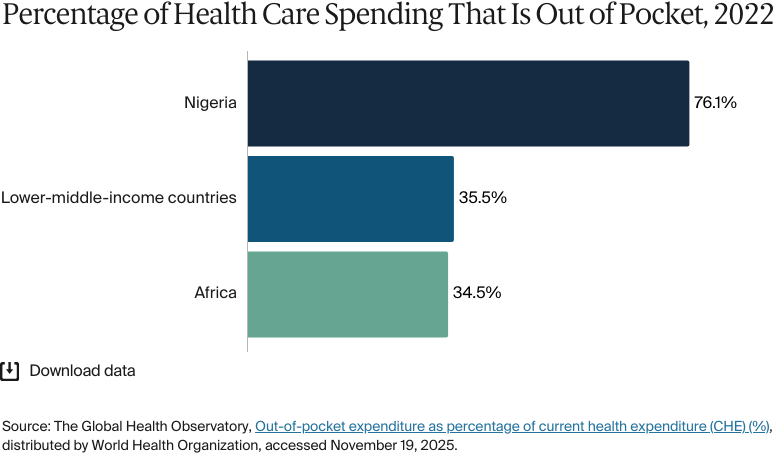
Health care provision in Nigeria is both public and private, with governance managed at the federal, state, and local levels. The health system is financed through a combination of general taxation, government funding, and out-of-pocket payments — the last of which account for 76 percent of total health spending. Health care is not universally free at the point of service, which can strain the population (about 91% were uninsured as of 2024).1 Following the implementation of the National Health Insurance Authority Act in 2022, Nigeria has renewed its commitment to providing universal health coverage by 2030 by mandating that all Nigerians participate in health insurance.2
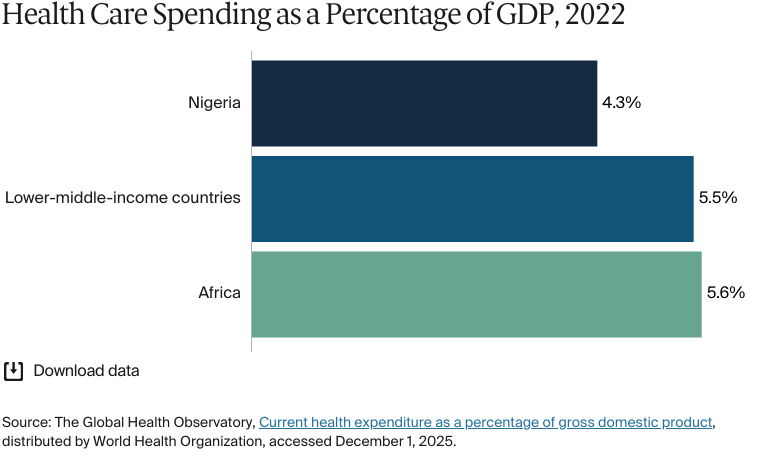
In 2023, Nigeria spent 3.86 percent of its gross domestic product on health care — higher than Ghana (3.7%) but below the 5.5 percent average for lower-middle-income countries.3 Although this is below the 15 percent target set by the 2001 Abuja Declaration for African Union countries, Nigeria has seen some improvements in care.4 Average life expectancy has increased by 10 years since 2000, reaching 64.5 years in 2023.5 However, Nigeria continues to face challenges, including a maternal mortality rate nearly double the African average, a limited health care infrastructure and the migration of skilled health care workers to other countries.
Nigeria is working toward universal health coverage, but funding constraints, workforce shortages, rapid population growth, and gaps in health care infrastructure (particularly in rural areas) pose ongoing challenges to the system.
Public insurance coverage: 9%
Private insurance coverage: 2%
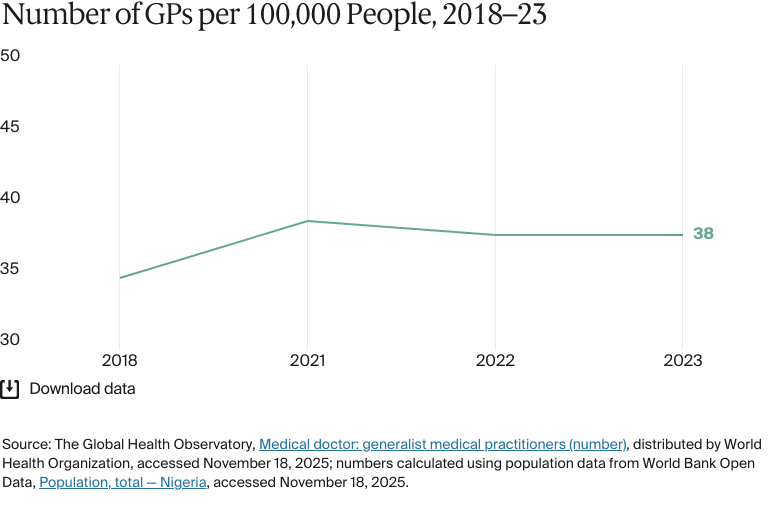
Primary care physicians: 38 per 100,000 people
Specialist physicians: N/A
In 2022, total health expenditure in Nigeria was USD 16.6 million. The government’s spending accounted for USD 2.2 billion, USD 11.3 billion came from out-of-pocket payments, and USD 2.7 billion came from international development aid.
Pharmaceutical spending: N/A
Out of pocket spending: 70.9% of total health care spend
Socioeconomic divides are a critical problem for Nigeria. Nigeria’s health care system is characterized by a disparity between wealthy Nigerians who have access to world-class private health care and those who don’t.
Political instability is one cause of health inequity in Nigeria. Over 87 percent of citizens living in poverty reside in Nigeria’s northern region, with about half concentrated in the north-west. Ongoing conflict between farmers and herders has exacerbated poverty by damaging people’s livelihoods.
In 1999, Nigeria established the National Health Insurance Scheme (NHIS) under Decree 35 of the 1999 Constitution, though enrollment did not begin until 2005. The NHIS aimed to achieve universal coverage by 2015 through a three-way partnership between the government, private health insurers, and health care providers. However, the voluntary nature of the program limited coverage to public-sector and organized private-sector workers.6 As a result, by 2021, only 5 percent of Nigerians were enrolled.7
To address these challenges, the NHIS was replaced by the National Health Insurance Authority (NHIA) in 2022. The NHIA introduced mandatory health insurance for all citizens and legal residents, intending to promote, regulate, and integrate health insurance programs to achieve universal health coverage by 2030.8
Nigeria’s public health care system is decentralized, with responsibilities shared among federal, state, and local governments.9 The 2014 National Health Act (NHA) provided mechanisms to mobilize resources from public, private, and philanthropic sources to fund a basic package of primary health care services. State governments have since developed their primary health care development agencies, supported by the National Primary Health Care Development Agency (see Primary Care).10
Nigeria is working toward universal health coverage, but funding constraints, workforce shortages, rapid population growth, and gaps in health care infrastructure (particularly in rural areas) pose ongoing challenges to the system.11 The government has introduced policies and made investments to address these challenges:
The National Policy on Health Workforce Migration aims to retain and attract health professionals through incentives, such as tax breaks and improved working conditions (see Physician Education and the Workforce).12
The National Health Sector Renewal Investment Initiative seeks to expand health insurance coverage and strengthen primary health care.13
The Vulnerable Group Fund was established to support 83 million indigent Nigerians and reduce reliance on out-of-pocket payments (see Addressing Health Inequities).
The private sector has also played a role. For example, the Presidential Initiative for Unlocking the Healthcare Value Chain (PVAC) secured USD 2 billion in foreign investment, supporting 74 health care projects (see Integration and Care Coordination).14
The Role of Public Health Insurance
The NHIA mandates that every legal resident enroll in health insurance, a change from voluntary participation under the NHIS. Unemployed citizens (33% of the total population) and self-employed citizens (81% of the employed population), meanwhile, were not covered under the NHIS.15 Including these groups under the NHIA expands the population covered by Nigeria’s public health insurance.
Enshrined in the NHA, the Basic Health Care Provision Fund (BHCPF) provides a minimum package of health care services for everyone with public health insurance. BHCPF is funded by an annual government grant of no less than 1 percent of the Consolidated Revenue Fund (the primary account for all federal government revenue), grants from international donor partners, contributions from the private sector, and contributions from other sources.16 The NHIA, in collaboration with the state health programs, is responsible for implementing the BHCPF.
Assistive devices, including prosthetics, produced in Nigeria
Basic mental health care (counselling)
Basic dental care, including fillings and simple extractions
Essential prescription drugs, with a 10 percent copayment.18
Services that are not covered include:
Specialist mental health care
Palliative care
Long-term care
Rehabilitative care
Home visits.
Safety Nets
The NHIA Act created the Vulnerable Group Fund, which subsidizes the cost of health care services for children under age 5, pregnant women, elderly people, people with physical or mental disabilities, and people with low income — individuals who earn NGN 70,000 (USD 46) or less per month.19
In addition to the NHIA, state health insurance programs provide Nigerians with financial assistance to avoid catastrophic health expenses. State governments typically contribute a percentage of their overall revenues to these programs to fund premiums for poor and marginalized citizens.20
These initiatives are designed to improve access to health care, but many Nigerians, particularly those in low-income and informal employment, still face financial challenges when seeking medical care. Coverage remains limited, especially among informal-sector workers, who may encounter difficulties with enrollment and affordability. Out-of-pocket health care expenses remain high, with individuals covering 75 percent of health care costs as of 2021 (see Cost Sharing and Out-of-Pocket Spending). Even in states with active insurance programs, participation rates have been relatively low, and factors such as administrative inefficiencies, fraud risks, and funding constraints pose challenges to the long-term sustainability of these programs.21
The Role of Private Health Insurance
Private health insurance is another source of health financing and is responsible for about 60 percent of health care service delivery.22 Only about 2 percent of Nigerians have private insurance due to the high cost of premiums.23
Individuals or employers can purchase private health coverage through health maintenance organizations or insurance companies.24 Health insurance provides financial coverage for medical expenses and can be purchased individually or through employers. Health maintenance organizations, on the other hand, offer managed health care services through a network of providers, often negotiating discounted rates to make care more affordable.25 They coordinate care within a set provider network and operate on a prepaid model.26 Both provide quicker access to quality care at private clinics, hospitals, diagnostic centers, and specialist treatment facilities.27
The Role of Government
The Federal Ministry of Health is responsible for tertiary health care (see Overview of the Delivery System for definitions) and establishes the country’s health policies. It provides specialized services through teaching hospitals, federal medical centers, specialist hospitals, and medical research institutes.
Nigeria’s state governments provide secondary health care through state general hospitals and occasionally provide tertiary care through state-owned teaching hospitals. State governments also coordinate the implementation of primary health care at the local level, adapt national policies and strategies to meet population needs, and lead the implementation of the country’s HIV/AIDS, tuberculosis, and malaria programs.
Nigeria has 774 local government areas, each administered by a council that oversees private, traditional, and alternative health care providers.28 These councils are also responsible for ward and village health committees, which promote health awareness and facilitate access to health care services.
Integration and Care Coordination
There is a lack of integration between public and private providers, which is a problem because private providers play an important role in the Nigerian system.
The government is taking steps to build public-private partnerships to bridge gaps in care and create a more resilient system. In 2023, the PVAC was established to generate private-sector opportunities to support overall health care delivery, promote cross-ministerial collaboration, and restructure health services.29 By the end of 2024, the PVAC had facilitated partnerships between the government, NGOs, and other industry players, with a USD 5 billion project pipeline for Nigerian health care innovation and USD 2 billion in foreign investment secured.30
Operations and Resources
Overview of the Delivery System
Public and private providers in Nigeria fall into four groups:
Primary care is typically a patient’s first point of contact and is provided by local facilities. Services include disease prevention, maternal and child care, immunization, nutrition education, and basic treatment of common illnesses.
Secondary care is planned or elective care that’s usually provided in hospitals. This includes more specialized services, such as general surgery, obstetrics, and treatment for more complex conditions.
Tertiary care is highly specialized care that’s offered at specialist and teaching hospitals. Services include advanced diagnostic and therapeutic services, complex surgeries, and treatment of rare and/or severe conditions.
Community-based care is an essential health service delivered by community health workers in local communities, particularly in rural and underserved areas.
Payments to health providers vary according to the level of care they provide. In primary care, capitation is the standard approach, in which providers receive a set amount for every patient under their care, regardless of how many services they use. In secondary and tertiary care, there’s a fee-for-service model, meaning providers are paid based on the specific services they provide to patients.31
Primary Care
Nigeria has about 30,000 primary health care facilities, but only 20 percent are fully functional due toinadequate funding, poorly maintained facilities, and staff shortages.32 As such, long working hours for doctors are a critical issue in the country. In 2022, resident doctors worked an average of 106.5 hours per week.33 Some institutions, such as the Duchess International Hospital, also have urgent 24-hour family medicine and general practitioner (GP) clinics.34
There is no definitive information available on whether Nigerian citizens are required to register with a primary care practice.
In 2023, Nigeria had 38 doctors for every 100,000 people, more than in nearby Côte d’Ivoire and Ghana (17 and 27 for every 100,000, respectively).35 In 2024, the Nigerian Medical Association warned that the country might lose 50 percent of its health care workforce by 2025. A main cause for concern is the many health care workers leaving the country in search of better economic and career opportunities, as well as better standards of living.36 There are no data available for the percentage of doctors employed publicly versus privately.
Dr. Adepeju Adeniran, who is the founder and co-chair of the nonprofit organization Women in Global Health, is more positive about communities’ roles in primary health care. “The bulk of the health care system is assessed by the public through the primary health care system, and there’s a huge component of community closeness and endorsement of health delivery in the primary health care system. That ownership of the health care system is very positive,” she says.
Community-based care is essential in reducing barriers to quality care, improving primary health care services, and increasing the uptake of health interventions. The Ward Health Development Committees, for example, aim to combat misinformation and ensure that communities have access to accurate health information. Additionally, sustainable health financing models, such as community-based health insurance programs, make medical services more affordable and reduce out-of-pocket costs.37
Outpatient/Specialist Care
Outpatient specialist care is provided by public and private hospitals. There are no data available for the number of outpatient specialist physicians or the proportions employed in public and private facilities.
Patients can be referred for outpatient specialist care by primary health care providers. However, many patients self-refer to secondary and tertiary facilities: between 60 and 90 percent of patients are reported to bypass primary health care in favor of secondary or tertiary facilities, meaning that specialists often treat minor ailments that are more suited to a primary health care setting.38 This leaves hospitals overstretched, with less time to treat more complex medical conditions.
Physician Education and the Workforce
About 3,500 medical doctors graduate annually from accredited medical colleges in Nigeria — about 1.6 for every 100,000 people.39 In 2023, the country had 37 fully accredited and seven partially accredited medical colleges.40
As of October 2023, the average monthly salary for a doctor employed by the federal government was NGN 240,000 (USD 313), and doctors employed by state governments earned less. Poor wages and working conditions have led to regular labor strikes and extended wait times in Nigerian hospitals.41
The country needs roughly 240,000 doctors.42 However, only about 72,000 doctors are registered with the Nigerian Medical Association.43This translates to 38 medical doctors for every 100,000 people, with the vast majority being primary care physicians.44
One reason for the shortage of health care professionals is an ongoing brain drain. At least 2,000 Nigerian doctors emigrate to countries such as the U.S., the U.K., and Canada each year. A 2018 survey revealed that 80 percent of Nigerian doctors had sought employment abroad.45
We’ve had the brain drain for more than 30 years. I remember being in medical school and seeing the first set of my seniors and early medical talent moving to other countries. The motivations now go beyond just financial or remuneration [considerations] — people want a better life and an improvement of relevant medical skills for themselves.
Dr. Adepeju Adeniran
Founder and Co-Chair
Women in Global Health
Dr. Adeniran also says that medical education in Nigeria is among the cheapest in the world, when considering fees alone. The estimated total cost of a medical degree in Nigeria ranges from USD 5,000 to USD 20,000, but this varies between federal, state, and private universities. “The government subsidizes the public schools, and then many medical graduates often take their talent and go abroad,” says Dr. Adeniran. “So it feels like a capital flight investment that’s not reaping benefits, understandably.”
Hospitals
Responsibility for Nigeria’s public hospitals is split between the federal and state governments. Teaching hospitals, federal medical centers, specialty hospitals, and federal tertiary hospitals are supervised by the Hospital Services Division of the Federal Ministry of Health and Social Welfare.46 General hospitals that provide secondary care services are managed by state ministries of health.47
There are no recent data available for the number of hospital beds in Nigeria, but capacity is an issue.48 Low capacity is exacerbated by patients’ high level of self-referral to secondary and tertiary care for illnesses that could be treated in primary care (see Outpatient/Specialist Care).
In 2022, Nigeria had 165 nurses for every 100,000 people, higher than the African average of 113.49
Mental Health Care
In 2021, the proportion of Nigerians with mental health disorders was 9.6 percent — lower than the lower-middle-income-country average of 13.5 percent.50
The country lacks qualified mental health professionals: in 2020, Nigeria had fewer than 300 psychiatrists — just 0.1 psychiatrists for every 100,000 people — and most were based in urban areas.51 Increasing the pool of qualified psychiatric medical professionals is challenging because training is concentrated in eight neuropsychiatric hospitals.52 There are no data available for the number of mental hospital beds or the total number of mental health professionals.
The mental health care sector faces additional challenges, including gaps in policy enactment and enforcement, financing, research, training, and the integration of mental health care into primary health care systems. Affordability of services is also an issue: beyond counselling, mental health care is not covered under public health insurance. Some private insurance plans include mental health care, but the breadth of coverage varies widely.
Nigeria’s government is looking to improve these services. In 2023, the National Mental Health Act replaced the outdated Lunacy Act of 1958, which had long been criticized for its derogatory terminology and lack of clear definitions relating to mental health.53 The new law aims to establish a legal framework for mental health care and substance abuse care services while addressing how society manages mental health. Its main objectives are to:
Provide direction for a rational, coherent, and unified response to the delivery of mental health services.
Promote and protect the fundamental human rights of those suffering from mental health conditions.
Ensure that mental health services are integrated and effectively delivered.
Implement approved national minimum standards for mental health care.
Improve the rehabilitation of people with mental health conditions and their reintegration into the community.
Adopt a community-based approach to mental health care.54
Long-Term Care and Social Support
Nigeria’s growing population of older adults is increasing the need for long-term care. The formal support care sector for older adults is still developing. Currently, it’s dominated by informal care that’s provided by families in the home.55 There are many services available to care for older adults, including residential care homes, nursing homes, in-home care, day care, and caregiver and family member training.56
The Care of the People program provides conditional cash transfers to older adults and those suffering from chronic conditions (for example, HIV/AIDS), but it covers less than one in every 1,000 poor households.57
The National Policy on Ageing for Older Persons was ratified in 2021 to enhance the quality of life for the elderly, strengthen care institutions, and establish a data management system to support research on aging and meet evolving needs.58 As of January 2025, the policy has not been implemented.
Cost and Affordability
Health Care Spending Overview
In 2022, total health expenditure in Nigeria was USD 16.6 million. The government’s spending accounted for USD 2.2 billion, USD 11.3 billion came from out-of-pocket payments, and USD 2.7 billion came from international development aid.59
Of the Nigerian government’s total budget for the 2024 fiscal year, NGN 1.3 trillion (USD 779.9 million) — about 4.8 percent of the total — was allocated to the health sector.60 This falls short of the 15 percent annual spending target set by the heads of state for African Union member states in the 2001 Abuja Declaration.61
The Federal Ministry of Health and Social Welfare underspent its approved budget by 31 and 47 percent in 2018 and 2021, respectively. This underspending was caused by bureaucratic delays, poor budget execution, competing priorities, capacity constraints, and delays in the release of allocated funds, especially at the subnational level.62
When it comes to the funding challenge in the health sector, Dr. Adeniran says the root cause of underfunding is a lack of strong accountability systems and processes, especially in the primary health care setting. “I don’t like to use the word underfunded when talking about primary health care because it almost sounds like there’s no availability of funds, which isn’t the case,” says Dr. Adeniran. “Instead, it’s because the accountability systems and the measurement of that funding are not as robust as they need to be. The key is accountability and making sure the funds do what they’re supposed to do.”
Pharmaceutical Spending
Medicines account for up to NGN 6.6 trillion (USD 3.9 billion) of Nigeria’s total health care spend.63 More than 70 percent is imported. This reliance on foreign imports, along with the 2023 devaluation of the naira, the exit of multinational companies, and an overall lack of consistent pricing mechanisms and negotiation frameworks, has led to an increase in drug prices.64
For example, from 2022 to 2023, the price of antibiotics, such as Amoxil, increased by as much as 400 percent.65 In May 2024, the BBC reported that the cost of one patient’s medication rose from NGN 9,000 (USD 6) in 2023 to more than NGN 67,000 (USD 42) in 2024 — an increase of 644 percent.66
In 2024, the Minister of Health acknowledged that affordability has been an ongoing issue in Nigeria for over 40 years, adding that fewer than 10 percent of citizens have health insurance. The result is that most individuals pay out of pocket for health care, including medications (see Cost Sharing and Out-of-Pocket Spending).67
Currently, only 25 percent of Nigeria’s pharmaceutical needs are being met by local manufacturing. In May 2024, the National Agency for Food and Drug Administration and Control said that it was committed to lowering medicine costs (see How Are Costs Contained?). It emphasized the need to strengthen local pharmaceutical production, which could reduce reliance on imports and stabilize prices.68
Cost Sharing and Out-of-Pocket Spending
Out-of-pocket spending accounted for 70.94 percent of Nigeria’s health care expenditure in 2023, well above the average of 35.5 percent for lower-middle-income countries.69
Annual total health expenditure was USD 70 per capita in 2022. Of that, out-of-pocket expenditure was USD 48.70
Dr. Adeniran explained that the impact of out-of-pocket expenses can range from a slight inconvenience to a catastrophic burden.
Noncommunicable diseases are beginning to push families into catastrophic spending. This can be caused by just one case of diabetes in a family — and that’s just diabetes without diabetic complications such as amputation, blindness, and renal damage. Similarly, heart disease is leading to catastrophic spending.
Dr. Adepeju Adeniran
Founder and Co-Chair
Women in Global Health
How Are Costs Contained?
The National Agency for Food and Drug Administration and Control 5 plus 5 program is designed to address the cost of pharmaceuticals. It grants importers of locally producible drugs a five-year extension on their import licenses, during which they must either transition to local production or partner with local manufacturers. This policy has led to a 30 percent increase in the number of new pharmaceutical companies in Nigeria, reducing reliance on costly imports and driving down drug prices.71
The Ceiling 34 policy, meanwhile, bans the import of 34 drugs that can be produced locally. Nigerian pharmaceutical companies, including Emzor and Fidson Healthcare, are setting up facilities to produce antimalarial active pharmaceutical ingredients, thereby reducing the country’s reliance on imports and lowering costs.72
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
In 2023, average life expectancy was 64.5 years (compared with 63.9 in Western sub-Saharan Africa) — 63.1 years for men and 65.9 years for women.73
The top three causes of death in Nigeria in 2021 were:
Lower respiratory infections: 90 deaths per 100,000 people
Malaria: 84 deaths per 100,000 people
Diarrheal diseases: 70 deaths per 100,000 people.74
The overall maternal mortality rate in 2023 was 993 per 100,000 live births, compared with an average of 442 in Africa.75
The infant mortality rate in Nigeria was 60 deaths per 1,000 live births in 2023, compared with 43 across Africa.76
In 2021, the share of Nigeria’s population with mental health disorders was 10 percent, compared with an average of 14 percent in lower-middle-income countries.77
The suicide rate in Nigeria in 2023 was 3 deaths per 100,000 people.78
Guns are responsible for two deaths in every 100,000 people in Nigeria.79
There are about 3.4 million people with HIV/AIDS in Nigeria. About one-third receive treatment, while about 150,000 people die from the virus each year.81
Socioeconomic divides are a critical problem for Nigeria. The country had a Gini coefficient — a statistical measure of inequity — of 35.1 in 2018; as of 2024, the Gini coefficient averaged 38.2 across 165 countries.82 Nigeria’s health care system is characterized by a disparity between wealthy Nigerians who have access to world-class private health care and those who don’t.
Political instability is one cause of health inequity in Nigeria. Politically unstable environments hamper responses to health emergencies and lead to disease spread and mortality. In 2020, conflicts such as the Boko Haram insurgency and protests against police brutality led to a rise in COVID-19 cases.83
Political instability can also negatively impact health reforms. In 2021, nine years after it was launched, the Saving One Million Lives initiative was discontinued. The program aimed to reduce mortality for children under age 5 by targeting six health areas, including maternal and child health, polio and routine vaccination, and access to essential medicines. Governance fragmentation and frequent turnover of political leadership led to a lack of sustained political commitment, resulting in the program losing funding and momentum.84
Over 87 percent of citizens living in poverty reside in Nigeria’s northern region, with about half concentrated in the north-west. Ongoing conflict between farmers and herders has exacerbated poverty by damaging people’s livelihoods.85
Addressing Health Inequities
In March 2022, the Lancet Nigeria Commission identified the country’s biggest health care issues as ineffective use of resources, lack of robust population health and mortality data, insufficient financing for health care, poor deployment of available health funding, and critical population inequities.86
As with rural populations (see Health Outcomes), the urban poor tend to live in informal settlements that lack government recognition. In these communities, inadequate infrastructure and financial barriers limit access to proper health care. Cities, such as Lagos, Kano, Port Harcourt, and Abuja, suffer from overpopulation, unsafe drinking water, poor sanitation, inadequate housing, malnutrition, and a high burden of diseases, such as malaria.87
Food insecurity is a critical issue. In 2024, the government’s report estimated that nearly 32 million people across 26 of Nigeria’s states were food-insecure during that year’s lean season from June to August. That same year, 44 percent of children from the poorest urban families faced severe food poverty, compared with 17 percent from the richest families. Malnutrition increases the likelihood of wasting, a life-threatening condition.88
The government has programs in place to resolve some of the issues related to health inequities. For rural populations, the focus is on improving the quality of and access to care. The Johns Hopkins Center for Communication Programs led the Breakthrough ACTION Nigeria initiative to empower local communities to implement health care services tailored to their residents. The center provided initial training, supervision, and technical assistance to ward development committees, which are local groups responsible for community health care. Participating committees have purchased needed essential medical equipment and completed construction work or repairs in clinics.89
In addition, through the UNICEF-led Child Nutrition Fund launched in 2023, four Nigerian states are providing financial resources to address child malnutrition; nine others have pledged commitments to do so.90
Innovation and Reform
Health Care Innovation
Nigeria has developed several health policies and guidelines to expand access to quality health care.
Sector-Wide Approach
One way the Nigerian government hopes to improve health care delivery is by adopting a sector-wide approach (SWAp). All stakeholders — including government agencies, donors, and private providers — come together under a single policy framework in an effort to ensure alignment and efficient use of resources.91
While SWAp has been in place in Nigeria only since December 2023, other countries have seen the benefits of the approach. Ghana, for example, has increased immunization rates by 30 percent and reduced child mortality by 15 percent since implementing SWAp.92
Private-Sector Financing Models for Family Planning Services
Recent reforms have focused on using the private sector to improve family planning services in Nigeria. In Lagos State, partnerships with private providers have been incentivized through tax relief, commodity support, and equipment provision.93
Another innovative approach has been the integration of family planning services into health insurance packages under the Lagos State Health Scheme program in Lagos State. This public-private model uses government-supported health insurance to subsidize family planning services at nonprofit and for-profit facilities.94
Health Care Technology
The Nigeria Digital Health Initiative, introduced in 2024, aims to integrate technology into health care delivery to expand access and reduce inequities. Its goals include increasing the adoption of electronic health records (EHRs), creating a national health information exchange, and improving digital health literacy across the medical workforce and population.95
Electronic Health Records
Adoption rates for EHRs in Nigeria are estimated to be between 18 and 23 percent. There are several challenges preventing further uptake of the technology, including limited infrastructure, poor internet connectivity, and a lack of information technology skills within the medical workforce.96
Some states are moving faster to adopt EHRs. The Lagos State Smart Health Information Platform, for instance, consolidates patient data from different providers and facilities across the public and private sectors.97 However, Nigeria’s government is seeking to create a national, unified EHR platform that enables physicians to manage clinical and administrative data across all levels of the health care system. In 2024, the government established a committee to manage the design and deployment of this platform.98
Digital Health Innovation
Digital health care has the potential to bridge gaps in access caused by the concentration of facilities in urban areas.99 In 2023, Nigerian start-up company mDoc Healthcare integrated ChatGPT’s large language model into its virtual self-care coach, Kem. The artificial-intelligence-powered chatbot is designed to support individuals at risk of, or living with, chronic health conditions by providing guidance on healthy living and preventive care. The technology is currently being evaluated in a community trial to ensure its effectiveness and minimize biases common in large language models.100
The NIGCOMHEALTH platform, launched in 2023, is another example of digital health innovation. It allows patients in any location to book medical appointments and speak to physicians across the country.101
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Queen Ukpo, “Achieving universal health coverage in Nigeria through legislation: the National Health Insurance Authority Act, 2021,” SSRN, July 16, 2024, http://dx.doi.org/10.2139/ssrn.4898695.
↩
Tope M Ipinnimo et al., “The Nigeria National Health Insurance Authority Act and its implications towards achieving Universal Health Coverage.” Nigerian Postgraduate Medical Journal 29, no. 4 (October–December 2022):281–287, https://doi.org/10.4103/npmj.npmj_216_22; Abiodun Awosusi, “Nigeria’s mandatory health insurance and the march towards universal health coverage.” Lancet 10, no. 11 (2022):e1555–e1556, https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(22)00369-2/fulltext.
↩
7
Gbadegesin O Alawode and David A Adewole, “Assessment of the design and implementation challenges of the National Health Insurance Scheme in Nigeria: a qualitative study among sub-national level actors, healthcare and insurance providers,” BMC Public Health 21, no. 124 (January 11, 2021), https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-10133-5.
↩
8
Ipinnimo et al., “The Nigeria National Health Insurance Authority Act.”
↩
9
Ipinnimo et al., “The Nigeria National Health Insurance Authority Act.”
↩
10
Awosusi, “Nigeria’s mandatory health insurance.”
↩
Ifediba, “Nigeria’s has an ambitious plan”; Nigeria Health Watch, “Nigeria’s health sector in 2024.”
↩
13
Nigeria Health Watch, “Nigeria’s health sector in 2024.”
↩
14
Nigeria Health Watch ,“Nigeria’s health sector in 2024.”
↩
15
Ipinnimo et al., “The Nigeria National Health Insurance Authority Act.”
↩
16
“Basic Health Care Provision Fund (BHCPF),” National Primary Health Care Development Agency, accessed November 20, 2024, https://nphcda.gov.ng/bhcpf/.
↩
Bolaji S Aregbeshola and Samina M Khan, “Out-of-pocket payments, catastrophic health expenditure and poverty among households in Nigeria 2010.” International Journal of Health Policy and Management 7, no. 9 (2018):798–806, https://doi.org/10.15171/ijhpm.2018.19.
↩
23
Ibrahim Abubakar et al., “The Lancet Nigeria Commission: investing in health and the future of the nation.” Lancet 399, no. 10330 (March 19, 2022):1155–1200, https://doi.org/10.1016/S0140-6736(21)02488-0; Hezekiah O Shobiye et al., “Determinants and perception of health insurance participation among healthcare providers in Nigeria: a mixed-methods study.” PLoS One 16, no. 8 (August 4, 2021), https://doi.org/10.1371/journal.pone.0255206.
↩
Murtala A Ngabea and Moses I Durotoluwa, “The impact of health maintenance organizations in the implementation of the Nigeria National Health Insurance Scheme in the federal capital territory (Abuja), Nigeria.” The Nigerian Medical Journal 64, no.6 (November–December, 2023):759–72, https://doi.org/10.60787/nmj-64-6-332.
↩
27
Generis Global Legal Services, “An overview of the healthcare system in Nigeria.”
↩
Zainab A Ibrahim et al., “Influence of Basic Health Care Provision Fund in improving primary health care in Kano State, a descriptive cross-sectional study.” BMC Health ServicesResearch 23, no.885 (August 22, 2023), https://doi.org/10.1186/s12913-023-09708-w; Nigeria Health Watch, “Primary health care in Nigeria.”
↩
33
SA Balogun et al., “Nigerian resident doctors’ work schedule a national study.” Nigerian Journal of Clinical Practice 25, no. 4 (April 2022):548–56, https://doi.org/10.4103/njcp.njcp_1901_21.
↩
Fortune B Effiong et al., “The role of community-based approaches in achieving universal health coverage: addressing the Nigerian narrative.” Annals of Medicine & Surgery 85, no. 5 (May, 2023):1769–73, https://doi.org/10.1097/MS9.0000000000000443.
↩
38
Francis G Koce et al., “A qualitative study of health care providers’ perceptions and experiences of patients bypassing primary healthcare facilities: a focus from Nigeria.” Journal of Global Health Reports 4 (July 27, 2020), https://doi.org/10.29392/001c.14138.
↩
39
Paul T KingPriest et al., “A national perspective on exposure to essential surgical procedures among medical trainees in Nigeria: a cross-sectional survey and recommendations.” BMC Medical Education 23, no. 913 (2023), https://doi.org/10.1186/s12909-023-04847-4.
↩
Generis Global Legal Services, “An Overview of the Healthcare System in Nigeria.”
↩
48
Toluwalashe S Soyemi and Abdullahi T Aborode, “Shortage of hospital bed capacity and overcrowding in emergency tertiary healthcare centers in Nigeria.” Annals of Medicine & Surgery 82, (October 2022):104675, https://doi.org/10.1016/j.amsu.2022.104675.
↩
Yusuf H Wada et al., “Mental health in Nigeria: a neglected issue in public health.” Public Health In Practice 2 (November 2021):100166, https://doi.org/10.1016/j.puhip.2021.100166; Ofor C Chijioke et al., “Barriers and attitudes towards mental health services in Nigeria: a systematic review.” International Neuropsychiatric Disease Journal 21, no. 5 (July 15, 2024), https://doi.org/10.9734/indj/2024/v21i5445.
↩
Gerald O Ozota, “Nigeria mental health law: challenges and implications for mental health services.” South African Journal of Psychiatry 30 (April 19, 2024):a2134, https://doi.org/10.4102/sajpsychiatry.v30i0.2134.
↩
Oyeneyin B David et al., “Strengthening long-term care as a critical strategy for healthy ageing: a perspective from Nigeria.” International Journal of Gerontology & Geriatric Research 4, no. 1 (2020), https://www.sciresliterature.org/Gerontology/IJGGR-ID21.pdf; Juliet CD Ezulike et al., “Aging and caring: exploring older adults’ motivation for informal caregiving to other aging individuals in Nigeria.” Innovation in Aging 8, no. 4 (January 2, 2024):igad140, https://doi.org/10.1093/geroni/igad140.
↩
Rebecca Holmes et al., “Social Protection in Nigeria: An Overview of Programmes and Their Effectiveness” (Project Briefing, no. 59, Overseas Development Institute / UNICEF, September 2011), https://media.odi.org/documents/7324.pdf.
↩
58
Kingsley C Mbam et al., “Aging in Nigeria: a growing population of older adults requires the implementation of national aging policies.” The Gerontologist 62, no.9 (November 2022):1243–50, https://doi.org/10.1093/geront/gnac121.
↩
59
Institute for Health Metrics and Evaluation, Financing global health, distributed by IHME, accessed November 19, 2025, https://vizhub.healthdata.org/fgh/.
↩
Makuochi Okafor and Chigozie Ohaka, “I wan live long, but e dey expensive — high cost of drugs hit patients for Nigeria,” BBC News Pidgin, May 21, 2024, https://www.bbc.com/pidgin/articles/cyjjd1r09lgo.
↩
67
National Agency for Food and Drug Administration and Control, “High Cost of Medicines.”
↩
Institute for Health Metrics and Evaluation, GBD Compare, distributed by IHME, accessed November 19, 2025, https://vizhub.healthdata.org/gbd-compare/; overall firearm mortality is the aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
Kevin Croke and Osondu Ogbuoji, “Health reform in Nigeria: the politics of primary health care and universal health coverage,” Health Policy and Planning 39, no. 1 (January 2024):22–31, https://doi.org/10.1093/heapol/czad107.
↩
Abubakar et al., “The Lancet Nigeria Commission.”
↩
87
Alhaji A Aliyu and Lawal Amadu, “Urbanization, cities, and health: the challenges to Nigeria — a review,” Annals of African Medicine 16, no. 4 (October–December 2017):149–58, https://pmc.ncbi.nlm.nih.gov/articles/PMC5676403/.
↩
Demilade R Salam et al., “Electronic health record: an underutilized tool in Nigeria’s healthcare system.” Continental Journal of Applied Sciences 18, no. 2 (September 17, 2023), https://doi.org/10.5281/zenodo.8352514.
↩
97
“Data-driven partnerships: shaping health outcomes in Lagos today and tomorrow,” Lagos SHIP, accessed December 1, 2025, https://digitalhealthplatforms.ng/.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.