Italy’s national health system offers universal coverage to all European Union citizens and registered residents through a tax-funded public model, with services largely free at the point of use.1 The system guarantees access to a comprehensive package of essential health services: primary, hospital, mental health, and preventive care.
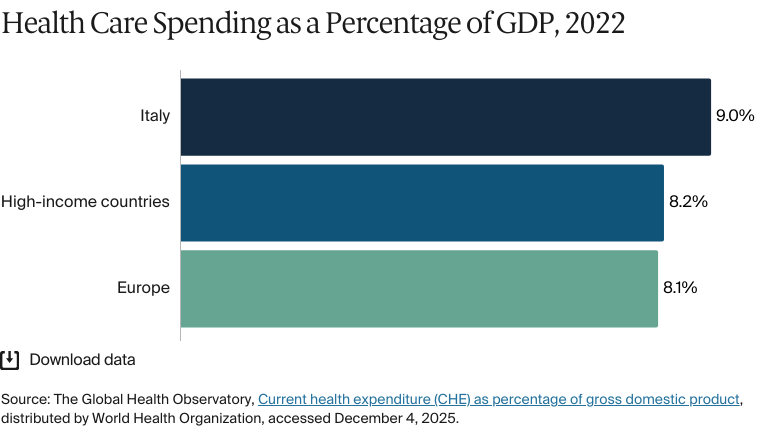
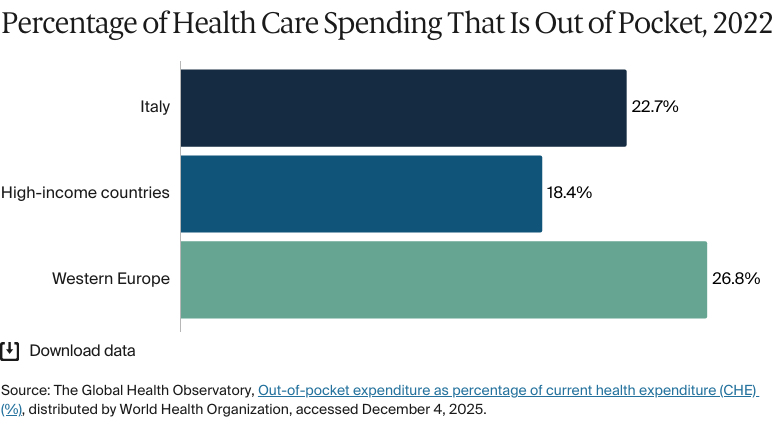
The system is highly decentralized; each of Italy’s 20 regions has its own agency responsible for planning, financing, and delivering care.2 To access treatment, individuals must hold a valid health insurance card or an equivalent card from another country in the European Union.3 Italy’s health system is predominantly publicly financed, and in 2023 health spending was about 8.4 percent of gross domestic product.4 Although most health services are free or subject to low copayments, out-of-pocket spending remains relatively high, driven by cost sharing for outpatient services, diagnostics, and branded pharmaceuticals.
Italy delivers comparatively strong health outcomes: Life expectancy is high (82 years), maternal and infant mortality rates are low, and the country has a longstanding emphasis on primary and preventive care. Still, workforce aging, long wait times, fragmented care coordination, and uneven access to services, particularly in the south of the country, pose barriers to equity and system sustainability.5
Italy’s national health system (Servizio Sanitario Nazionale, or SSN) was established in 1978. All citizens and resident foreign nationals have access to a wide range of publicly financed health services. The system is primarily funded through general taxation, with additional revenues from regional taxes and copayments.
Public insurance coverage: 100% of population
Private insurance coverage: 25% of population
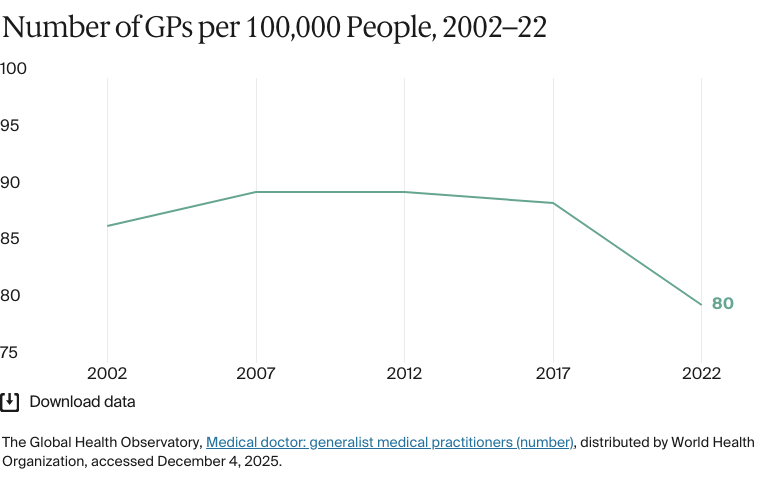
Primary care physicians: 80 per 100,000 people
Specialist physicians: 343 per 100,000 people
The system is predominantly publicly funded, with government expenditure accounting for 74 percent of total health spending in 2022. Per capita spending totaled USD 3,340.
Pharmaceutical spending: 17.5% of total health care budget
Out of pocket spending: 22.7% of total health care spend
There are persistent differences in health outcomes between the richer north and the poorer and less developed south, the latter of which has worse access to care and lower quality of services and life expectancy.
Migrants also experience worse health outcomes than Italian citizens. Nearly half (48%) of migrants lack access to health care services. Many do not know they have a right to care, and those who do often experience difficulties navigating administrative processes to access services. Migrants also have high levels of mental health issues, with 62 percent exhibiting signs of psychological distress.
Italy’s national health system (Servizio Sanitario Nazionale, or SSN) was established in 1978, replacing a fragmented social insurance with a universal, tax-funded public service that was modeled on the United Kingdom’s (U.K.) National Health Service.6
Initially centralized, the system suffered from inefficiencies due to unclear responsibilities, fragmented planning, and increased costs. This prompted reforms in the 1990s that decentralized control to autonomous local authorities and more independent hospital trusts. A 2001 constitutional reform further shifted financing and service delivery to individual regions, while the state retained stewardship over the Essential Levels of Care (Livelli Essenziali di Assistenza, or LEA), a national benefits package that defines guaranteed services for residents and citizens.7
Overall, the performance of the national health system over time has been very successful. If we look at some important outcomes, it has been very positive: improvement of life expectancy, reduction in avoidable mortality, amenable and infant mortality.
Professor Giovanni Fattore
Department of Social and Political Sciences
Università Bocconi
However, since the 2000s, an aging population and austerity have prompted strategies to contain costs, including hospital downsizing and a shift toward outpatient and community care.8 The COVID-19 pandemic exacerbated service backlogs, prompting renewed investment in digital tools, regional infrastructure, and staffing under the National Recovery and Resilience Plan funded by the European Union (E.U.) (see Addressing Health Inequities).9
The Role of Public Health Insurance
All citizens and resident foreign nationals have access to a wide range of publicly financed health services. The system is primarily funded through general taxation, with additional revenues from regional taxes and copayments.10
Documented migrants, asylum seekers, and beneficiaries of international protection are entitled to the same health services as Italian citizens upon registration with the SSN. Asylum seekers are registered and have access to care at the point of lodging an asylum application. Until they are registered, migrants only have access to emergency and essential care free of charge.11
Services covered by public health insurance are as follows:12
Dental care isn't generally covered, except for some services provided to children under age 14. Orthodontics and prosthetic devices are excluded.
Eye care isn't covered under the public benefits package.
Long-term care isn't covered through the health service. However, a separate national allowance is available for individuals with severe functional limitations (see Long-Term Care and Social Support).
Most essential services are provided with a low copayment or none at all. Exemptions from copayments are available based on income, age, chronic illness, and disability status (see Safety Nets). Regional authorities can offer additional services beyond those included in the LEA if they fund them independently.14
Safety Nets
The publicly financed health system includes a range of exemptions to reduce out-of-pocket costs for specific groups. These are based on income, having a chronic or rare health condition, age, and disability status. National guidelines exist, but the thresholds vary according to region.15
Children under age 6 and adults over age 65 who live in households with an income less than EUR 36,152 (USD 39,126) are fully exempt from outpatient copayments. Unemployed individuals and pensioners with dependent family members qualify for an exemption if their annual income is less than EUR 8,263 (USD 8,943).16
Individuals eligible for exemptions include those with severe disabilities, war-related injuries, blindness, deafness, or injuries sustained in public service.17 Anyone with a chronic or rare condition, including diabetes, chronic kidney disease, and thalassemia, is exempt from cost sharing for services related to diagnosis and ongoing management.18
In regions that apply copayments for prescription medications, exemptions are made based on income, age, employment, and disability status. These vary according to regional rules19(see Cost Sharing and Out-of-Pocket Spending).
The Role of Private Health Insurance
Private health care supplements the public health system. The way private health is funded — with employer contributions and indirect subsidies such as tax rebates — tends to favor people with higher incomes and stable employment.20 In 2023, 25 percent of Italians had some type of private insurance.21
There are three main categories of private health insurance:
Supplementary health funds, which don't involve risk selection and operate within the logic of the public system
Complementary health funds, which are eligible for tax benefits if at least 20 percent of their services cover items that aren't included in the public benefits package
For-profit private insurers, which offer broader coverage.22
The Role of Government
The health care system is governed through a decentralized model.23 At the national level, the Ministry of Health (Ministero della Salute) oversees health system planning and performance monitoring. It sets national health priorities, defines the essential benefits package, and monitors consistency with the constitutional guarantees of universal access and equity. It also defines funding criteria and the total health care budget, which is then allocated to the public by the Ministry of Economy and Finance (Ministero dell'Economia e delle Finanze, or MEF) through the National Health Fund (Fondo Sanitario Nazionale, or FSN).24
The Ministry of Health works in partnership with the following national agencies:
The Italian National Institute of Health (Istituto Superiore di Sanità, or ISS), which conducts research, surveillance, and technical guidance on public health issues
The Italian Medicines Agency (Agenzia Italiana del Farmaco, or AIFA), which regulates the pricing, approval, and use of pharmaceuticals
The National Agency for Regional Health Services (Agenzia Nazionale per i Servizi Sanitari Regionali, or Agenas), which supports quality monitoring, service planning, and interregional coordination
The National Institute for Insurance Against Accidents at Work (Istituto Nazionale per l’Assicurazione contro gli Infortuni sul Lavoro, or INAIL), which manages workplace injury prevention and rehabilitation services
The Institutes for Care and Scientific Research (Istituti di Ricovero e Cura a Carattere Scientifico, or IRCCS), national centers of excellence in research and specialized care, which the Ministry of Health cogoverns
Regional governments have substantial autonomy over health care planning, financing, and service delivery. They define regional health plans, manage the allocation of funds to providers, and organize networks of care. Within each region, local health authorities (aziende sanitarie locali, or ASL) are responsible for delivering primary care, preventive services, and hospital care. They also manage community services and coordinate with local governments to support social care integration.25
Health districts, operating under the ASL, directly deliver services to patients, manage commissioning, and maintain continuity across care settings.26
Integration and Care Coordination
A 2022 ministerial decree introduced community health centers (Case della Comunità, or CdC), home care coordination hubs (Centrali Operative Territoriali, or COT), and telemedicine to support integrated, local care delivery. Early evidence suggests that this has reduced avoidable hospitalizations, but workforce shortages and uneven digital adoption are barriers.27
The 2022 decree was part of the post-COVID National Recovery and Resilience Plan, which aimed to reduce unnecessary hospital use, strengthen preventive care, and support aging populations. Integrated care pathways help to coordinate hospital discharge with community-based follow-ups, especially for older adults and people with chronic needs.28
Operations and Resources
Overview of the Delivery System
The health system is structured into three levels of care:
Primary care includes general practice, family medicine, preventive health and community-based care.
Secondary care includes hospital-based and specialist outpatient services for more complex or nonurgent conditions. These services are provided through public hospitals, semiautonomous hospital trusts (aziende ospedaliere, or AO), and accredited private providers. Hospitals are funded through a combination of diagnosis-related group (DRG) payments for inpatient care, fee for service for outpatient services, and daily rates where appropriate.29
Tertiary care includes specialized treatment for rare and complex conditions. This is delivered by IRCCS, which also conducts clinical research, often for rare or complex conditions. Funding comes from regional and national budgets and includes DRG-based payments, along with dedicated financing for research and specialized care delivery.30
Primary Care
Primary care is the entry point to the health system and is managed by the ASL. All residents must register with a general practitioner (GP), or with a pediatrician for children under age 6, through their ASL.31
GPs are paid mainly through capitation, adjusted for age and geography, with fee-for-service supplements for services such as vaccinations and home visits.32 Out-of-hours care is provided by out-of-hours primary care physicians (medici di continuità assistenziale, or MCA), and urgent cases are handled via the national emergency call system.
In 2022, Italy had 80 GPs for every 100,000 people, a rate higher than in the U.K. (79) but lower than in Germany (105).33
Uneven distribution of GPs across regions has led to shortages, particularly in rural areas, where needs are high and services are limited.34 These concerns are compounded by the aging profile of GPs. In 2023, about 55 percent of doctors were over age 55, making the medical workforce one of the most senior in Europe.35
Outpatient/Specialist Care
Patients must obtain a referral from their GP to access specialist care. After receiving a referral, patients are able to choose any accredited provider within the national system.36
Regional disparities in wait times have widened, especially in the south, where long delays for specialist appointments are common.37 In addition, specialist care is still largely hospital-based, with limited integration between outpatient and primary care services affecting continuity of care for patients with complex or chronic conditions. This is a focus area addressed in the 2022 ministerial decree (see Integration and Care Coordination).38
In 2022, there were 343 specialist medical practitioners for every 100,000 people, below the average in Germany (350 in 2021).39
Physician Education and the Workforce
As of 2023, there were 22 medical universities.40 In 2024–25, there were 20,867 posts available for medicine and surgery. Of these, 19,467 were reserved for candidates from E.U. countries or from non-E.U. countries who are resident in Italy, while 1,400 were reserved for students from non-E.U. countries who are resident outside of Italy.41
As of 2022, under the National Recovery and Resilience Plan, more than 4,200 new specialization contracts had been added since the 2020–21 academic year.42
In 2023, there were 16.6 medical graduates for every 100,000 people, above the Organisation for Economic Co-operation and Development (OECD) average of 14.2 in 2021.43 However, just 26 percent of physicians are GPs, and the aging workforce is likely to create shortages.44
Efforts to strengthen the pipeline include doubling GP residency slots between 2018 and 2021 and expanding access to specialty training.45
Hospitals
BY THE NUMBERS
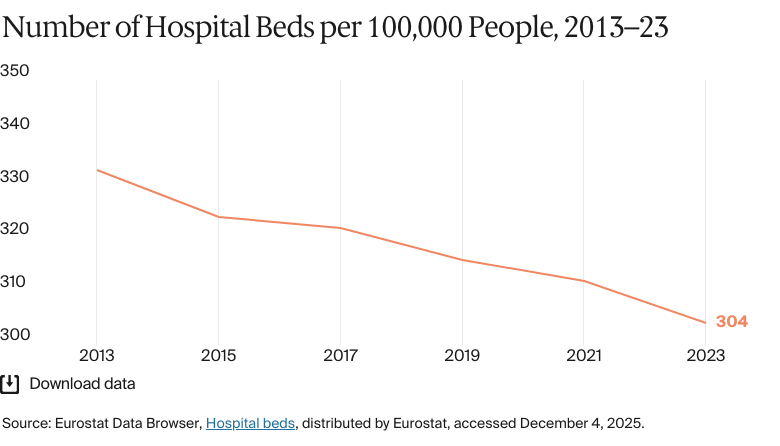
In 2023, there were 304 hospital beds per 100,000 people (compared with 510 across the E.U.).46
In 2022, there were 652 nurses per 100,000 people (compared with 826 across Europe).47
As of 2022, there were 996 hospitals, split between 511 public and 485 private accredited facilities.48 Public hospitals are managed by the SSN through ASL or autonomous hospital trusts, while private hospitals are integrated through accreditation agreements and focus on rehabilitation and residential care.49
Hospitals are funded regionally, mostly through DRGs for inpatient care, fee-for-service for outpatient services, and fixed budgets for emergency and intensive care.50
A 2015 ministerial decree introduced a hub-and-spoke model to centralize complex care in 43 hub hospitals and redistribute routine services to 112 spoke hospitals, with the goal of improving efficiency and continuity of care.51
As in much of the rest of Europe, the number of hospital beds has declined with the shift toward outpatient and community care.52 However, uneven regional implementation has led to significant patient mobility; in particular, patients are often moved from the south to better-resourced hospitals in the north.53
Mental Health Care
BY THE NUMBERS
There were six psychiatrists per 100,000 people in 2020, below the average of nine for high-income countries.54
In 2020, there were 43 mental health professionals per 100,000 people, below the average of 62 in high-income countries.55
The mental health system has been rooted in community-based care since the introduction of the Basaglia Law or Law 180 (Legge Basaglia or Legge 180) in 1978. This law abolished psychiatric hospitals and emphasized social integration.56 Patients typically access services via GP referral. Care is delivered through community mental health centers, hospital-based psychiatric wards, and residential facilities, with specialized services available for addictions and neurodevelopmental disorders.57
The Ministry of Health has promoted a number of initiatives to improve quality and access to care. For example, in 2023, a Technical Table for Mental Health (Tavolo tecnico per la salute mentale) was established to coordinate care pathways and promote intersectoral collaboration.58 Meanwhile, the Psychologist Bonus (Bonus psicologo), which was made permanent in 2023, aims to improve access through income-based subsidies for those requiring psychological support (see Safety Nets).59
In 2020, there were 43.3 mental health professionals for every 100,000 people.60 There are no current data available for the number of mental hospital beds.
Long-Term Care and Social Support
The long-term care system provides residential, semi-residential, and home-based services through a decentralized model that's funded publicly and privately. There's no dedicated long-term care insurance program, but a universal cash allowance (indennità di/accompagnamento) is provided to individuals with severe functional limitations regardless of income status. In 2022, the allowance was EUR 525 (USD 568) per month.61
Residential health facilities (residenze sanitarie assistenziali) provide residential care for older adults and people with dementia, with costs shared among the SSN, municipalities, patients, and the National Institute for Social Security (Istituto Nazionale della Previdenza Sociale, or INPS).62 The SSN also funds home care services, including medical support, home hospitalization, and semi-residential day centers (centri diurni integrati).63
The system faces growing pressure from workforce shortages, a reduction in family caregiving, and an aging population.64 Regional disparities and reliance on private providers complicate access, prompting calls for standardization, increased public investment, and workforce expansion.
Cost and Affordability
Health Care Spending Overview
In 2023, 8.4 percent of GDP was spent on health care, slightly above the average of 8.1 percent for high-income countries in 2023.65
The system is predominantly publicly funded, with government expenditure accounting for 74 percent of total health spending in 2022. Per capita spending totaled USD 3,340.66
Pharmaceutical Spending
In 2024, pharmaceuticals accounted for 17.5 percent of total health care spending. Per capita spending was USD 905 in the same year.67
The government has implemented a number of cost-containment measures. Since 2001, public drug reimbursement has been capped at the generic price, requiring patients to pay the difference for branded drugs.68 While the market share of generic drugs has nearly doubled within a decade, reaching 27 percent in 2021, it’s lower than in many European countries.69 In 2021, retail drug copayments totaled EUR 1.5 billion (USD 1.6 billion), over 73 percent of which came from premiums on branded drugs.70
AIFA evaluates drugs based on their therapeutic value and cost-effectiveness.71 Regions can adopt additional measures, such as direct distribution and targeted copayments, but as of 2023, nine regions had no drug copayment in place.
Cost Sharing and Out-of-Pocket Spending
In 2022, per capita out-of-pocket spending was USD 713, above the average of USD 556 in high-income countries.72 Primary care is free at the point of use. However, copayments apply to many outpatient services and diagnostic tests. These are typically capped at about EUR 36 (USD 39) per service group.73
For prescription drugs, patients generally pay a charge per package that varies according to region and whether it's a branded product (see Pharmaceutical Spending).74
Exemptions apply to certain groups according to age, income, and health status (see Safety Nets). Services such as cancer screening, HIV/AIDS testing, and organ donations are free to everyone.75
There's no annual cap on copayments.76 Regional variations in copayment policies mean that financial protection is inconsistent across the country.
How Are Costs Contained?
There's a mix of national and regional cost-containment measures to manage health spending, particularly in pharmaceuticals and hospital services.
At the national level, annual spending caps on reimbursed drugs are tied to the health care budget. In 2024 and 2025, this was 15.3 percent, split between retail-distributed drugs (6.8%) and hospital-procured drugs (8.5%). A payback system obliges pharmaceutical companies to refund any excess expenditure, effectively controlling public spending on drugs but creating market distortions that have potential consequences in regard to access, equity, and innovation.77
Regions that exceed health spending targets are required to adopt mandatory recovery plans. These measures have typically included hospital bed reductions, staffing freezes, and expanded outsourcing to private providers. Between 2007 and 2019, recovery plans helped to eliminate the SSN’s overall deficit.78 However, those regions under recovery plans (mainly regions in the south), have faced longer wait times, lower investment, and reduced access to services.79 Studies show that these areas have worse health outcomes.80
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
In 2021, average life expectancy was 82 years (compared with 80 in high-income countries) — 80 years for men and 84 years for women.81
The avoidable mortality rate was 145 deaths per 100,000 people in 2022, compared with 237 across OECD countries in 2021.82
The top three causes of death in 2021 were:
Ischemic heart disease: 148 deaths per 100,000 people
The maternal mortality rate was 7 deaths per 100,000 live births in 2023 (compared with 11 on average in Europe).84
The infant mortality rate was 2 deaths per 1,000 live births in 2023 (compared with seven on average in Europe).85
In 2021, the share of the population with mental health disorders was 17 percent (compared with 16% on average in high-income countries).86
The suicide rate was 7per 100,000 people in 2023, lower than the average of 12 per 100,000 people across high-income countries.87
Guns are responsible for one death in every 100,000.88
17 percent of adults were affected by obesity in 2022.89
Life expectancy is above the average for high-income countries, and maternal and infant mortality rates are below the average for high-income countries.90 The suicide rate is also comparatively low.91
The avoidable mortality rate was on a downward trend from 2015 to 2019, though it spiked from 136 to 163 avoidable deaths for every 100,000 people in 2020, likely because of the COVID-19 pandemic. The rate has continued to fall since but remains above pre-pandemic levels. In 2022, there were 145 avoidable deaths for every 100,000 people, considerably below the average of 237 across OECD countries in 2021.92
Addressing Health Inequities
Disparities in health care access and outcomes across certain regions and populations are longstanding.93 There are persistent differences in health outcomes between the richer north and the poorer and less developed south, the latter of which has worse access to care and lower quality of services and life expectancy. “There is a strong perception that the [national health system] is no longer able to provide universal coverage in an equitable way and reduce geographical disparities. I've been working in this field for 30 years. I've never seen a phase like this, where there's a general claim that the [national health system] cannot survive in this way,” says Giovanni Fattore.
Citizens from southern regions are more likely to report unmet medical needs, and there are persistent gaps in access and outcomes; northern regions offer broader service availability and shorter wait times.94 Calabria, Campania, and Sicily in the south have higher levels of years of life lost to diseases such as stroke, Alzheimer's disease, and lung cancer.95
Since patients are free to choose their medical providers, people from the south often seek care in northern and central regions, which receive more resources owing to their older populations.96
Inequities in education also affect health outcomes. In 2018, for example, there was a three-year difference in life expectancy between educated and less-educated men. These differences were more pronounced in southern regions.97
Migrants also experience worse health outcomes than Italian citizens. Nearly half (48%) of migrants lack access to health care services. Many do not know they have a right to care, and those who do often experience difficulties navigating administrative processes to access services. Migrants also have high levels of mental health issues, with 62 percent exhibiting signs of psychological distress.98
Several national initiatives have aimed to address these gaps. The 2020 New Guarantee System (Nuovo Sistema di Garanzia, or NSG), for instance, evaluates regional compliance with the LEA.99
The 2020–25 National Prevention Plan (Piano Nazionale della Prevenzione, or PNP), meanwhile, was developed by the Ministry of Health in collaboration with regional governments to address regional and socioeconomic health inequities. The plan aims to promote well-being, reduce the burden of chronic disease, and improve the uptake of preventative interventions, such as screening and vaccinations, among at-risk groups.100
In addition, targeted investments through the National Recovery and Resilience Plan, implemented in 2021 as part of the E.U.’s Next Generation E.U. program, aim to reduce regional and social inequities in care access by fostering a preventive, community-based care model.101
Innovation and Reform
Health Care Innovation
Reforms have prioritized infrastructure upgrades, care model redesign, and digital health integration, particularly under the National Recovery and Resilience Plan, which allocated EUR 16 billion (USD 17 billion) to health care modernization through 2026. Notable initiatives include the development of community-based care, the restructuring of hospital networks, and the expansion of digital tools and telemedicine.102
While there have been reforms and investments in new care models, the system isn't especially innovation-driven. “There’s no national agency for innovation in health care, and regions often interpret policies differently,” says Giovanni Fattore. Innovation in the health care system tends to be reactive, prompted by crisis (such as the COVID-19 pandemic) rather than embedded in a long-term strategy.103 Initiatives such as telemedicine and care coordination expanded rapidly during the pandemic in response to immediate needs, but maintaining momentum has been difficult.104
Health Care Technology
Italy has made progress in digitalizing health care delivery, with investments in telemedicine, electronic health records, and appointment management systems. Accelerated by the COVID-19 pandemic, telemedicine is now formally integrated into the SSN. Teleconsultations and telemonitoring are delivered through a national cloud infrastructure that is improving access in remote and underserved areas.105
The electronic health record system (Fascicolo Sanitario Elettronico, or FSE) allows patients and providers to access integrated health data, including prescriptions, diagnostic test results, and hospital records.106 Many private providers aren’t able to upload data automatically, however, and regional variation in technical standards limits interoperability.107 As part of the National Recovery and Resilience Plan, the FSE 2.0 seeks to build on existing data infrastructures, with a view to all regions using it by 2026.108
The National Plan for the Governance of Waiting Lists (Piano Nazionale di Governo delle Liste di Attesa, or PNGLA), updated in 2019, introduced centralized online booking and tracking to reduce delays to outpatient and diagnostic services. Meanwhile, electronic prescriptions are standard nationwide, and the use of digital COVID-19 certificates helped to build the infrastructure for other digital health tools.109
In 2025, the government approved a national artificial intelligence (AI) bill. The law specifies that AI should be used to support, not replace, medical practitioners in the prevention, diagnosis, and treatment of patients. To align with informed consent standards, it mandates that patients must be informed when AI is used in their care.110
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Sarah Humboldt-Dachroeden, “A governance and coordination perspective: Sweden's and Italy's approaches to implementing One Health.” SSM: Qualitative Research in Health 2 (December 2022):100198, https://doi.org/10.1016/j.ssmqr.2022.100198.
↩
De Belvis et al., Italy: Health System Review 2022.↩
27
Matteo Maria Cati, “The new health district: reshaping the Italian health system,” Biomedical Journal of Scientific and Technical Research 51, no. 5 (July 2023), https://doi.org/10.26717/BJSTR.2023.51.008157; Christian J. Wiedermann et al., “Examining South Tyrol’s experience: Digital health adoption and workforce issues in implementing Italy’s primary care reform under ministerial decree no. 77/2022,” Epidemiologia 5, no. 4 (2024), https://doi.org/10.3390/epidemiologia5040057.
↩
28
De Belvis et al., Italy: Health System Summary 2024.↩
29
De Belvis et al., Italy: Health System Summary 2024.↩
30
De Belvis et al., Italy: Health System Summary 2024.↩
Maria Gabriella Melchiorre et al., “Frail older people ageing in place in Italy: Use of health services and relationship with general practitioner,” International Journal of Environmental Research and Public Health 19, no. 15 (2022), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9332283.
↩
35
European Observatory on Health Systems and Policies, Italy: Country Health Profile 2023.
↩
World Health Organization, Member State Profile.
↩
56
De Belvis et al., Italy: Health System Review 2022.↩
57
De Belvis et al., Italy: Health System Review 2022.↩
58
“Technical working group on mental health” (Tavolo di lavoro tecnico sulla salute mentale), Ministry of Health (Ministero della Salute), last updated December 20, 2024, https://www.salute.gov.it/new/it/tema/salute-mentale/tavolo-di-lavoro-tecnico-sulla-salute-mentale (a brief description of the composition and purpose of the mental health working group established in Italy by ministerial decree in 2023).
↩
59
De Belvis et al., Italy: Health System Summary 2024.↩
60
World Health Organization, Member State Profile.
↩
61
De Belvis et al., Italy: Health System Review 2022.↩
62
De Belvis et al., Italy: Health System Review 2022.↩
63
De Belvis et al., Italy: Health System Review 2022.↩
64
De Belvis et al., Italy: Health System Review 2022.↩
65
Eurostat, Health care expenditure by financing scheme;The Global Health Observatory, Current health expenditure.↩
66
Institute for Health Metrics and Evaluation, Italy, all-cause spending as % of total health spending, 2022–2022, distributed by IHME, accessed December 4, 2025, http://ihmeuw.org/7bkh.
↩
“Suicide Rate by Country 2026”,World Population Review, accessed January 21, 2026, https://worldpopulationreview.com/country-rankings/suicide-rate-by-country
↩
88
Institute for Health Metrics and Evaluation, GBD compare, distributed by IHME, accessed December 4, 2025, https://vizhub.healthdata.org/gbd-compare/; overall firearm mortality is an aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
The Global Health Observatory, Life expectancy; The Global Health Observatory, Maternal mortality; figures calculated using data from IstatData, “Italian National Institute of Statistics data warehouse”; The Global Health Observatory, Infant mortality.↩
OECD Data Explorer, Avoidable mortality; Organisation for Economic Co-operation and Development, Health at a Glance.↩
93
Organisation for Economic Co-operation and Development and European Observatory on Health Systems and Policies, Italy: Country Health Profile 2021.
↩
94
De Belvis et al., Italy: Health System Review 2022; Fattore, interview.
↩
95
Mohsen Naghavi, “State of health and inequalities among Italian regions from 2000 to 2021: a systematic analysis based on the Global Burden of Disease Study 2021,” The Lancet Public Health 10, no. 4 (April 2025):e309–e320, https://doi.org/10.1016/S2468-2667(25)00045-3.
↩
96
De Belvis et al., Italy: Health System Review 2022.↩
97
De Belvis et al., Italy: Health System Review 2022.↩
De Belvis et al., Italy: Health System Review 2022.↩
100
“National Prevention Plan 2020–2025” (Piano Nazionale della Prevenzione 2020–2025), National Institute of Health (Istituto Superiore di Sanità), September 10, 2020, https://www.epicentro.iss.it/piano_prevenzione/pnp-2020-25; “The ‘National Prevention Plan 2020-2025,’ adopted by the State-Regions Agreement on August 6, 2020, represents the fundamental central planning tool for prevention and health promotion interventions to be implemented throughout the country”.
↩
101
Organisation for Economic Co-operation and Development and European Observatory on Health Systems and Policies, Italy: Country Health Profile 2021.
↩
102
De Belvis et al., Italy: Health System Summary 2024.↩
Fidelia Cascini et al., “A new digital model for the Italian Integrated Home Care: strengths, barriers, and future implications.” Frontiers in Public Health 11, no 1292442 (November 2023), https://doi.org/10.3389/fpubh.2023.1292442; De Belvis et al., Italy: Health System Review 2022.↩
106
Giulia Re Ferrè, Digitalizing Healthcare in Italy and Germany: The Electronic Health Record and m-Health Regulation as Key for e-Health (Interdisciplinary Research Center on Public Administration Law [Centro di Ricerca Interdisciplinare sul Diritto delle Amministrazioni Pubbliche], January 29, 2024), https://doi.org/10.13130/2723-9195/2024-1-14.
↩
Francesco Andrea Causio et al., “Fragmented but evolving: a response to the editorial ‘The Italian health data system is broken’.” The Lancet Regional Health: Europe 51, no. 101256 (March 2025), https://doi.org/10.1016/j.lanepe.2025.101256.
↩
109
De Belvis et al., Italy: Health System Summary 2024.↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.