Canada’s publicly funded health care system, Medicare, provides coverage to all citizens and permanent residents. It does this through 13 provincial and territorial insurance plans that must meet the federal standards set out in the Canada Health Act (Loi canadienne sur la santé). The system is mainly financed through the tax system and federal government funding.
All permanent residents are entitled to medically necessary hospital and physician services without paying out of pocket. But it’s up to the provincial and territorial governments to decide which services are medically necessary and, therefore, covered. As a result, access to certain services — particularly dental care, eye care, and prescription drugs — varies across provinces. Depending on where they live, residents may need to purchase supplementary private health insurance or pay out of pocket.
Canada provides universal health care through Medicare, which covers all medically necessary health services for Canadian citizens and permanent residents. Any eligible individual can apply for public health insurance within their province or territory and receive a health card that entitles them to non-emergency health services at public medical facilities.
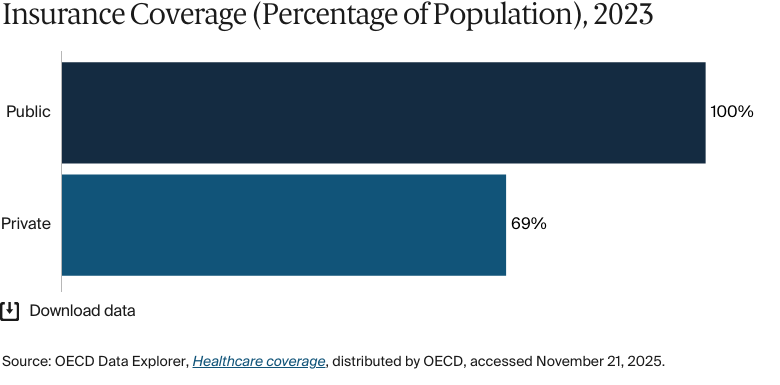
Public insurance coverage: 100% of population
Private insurance coverage: 69% of population
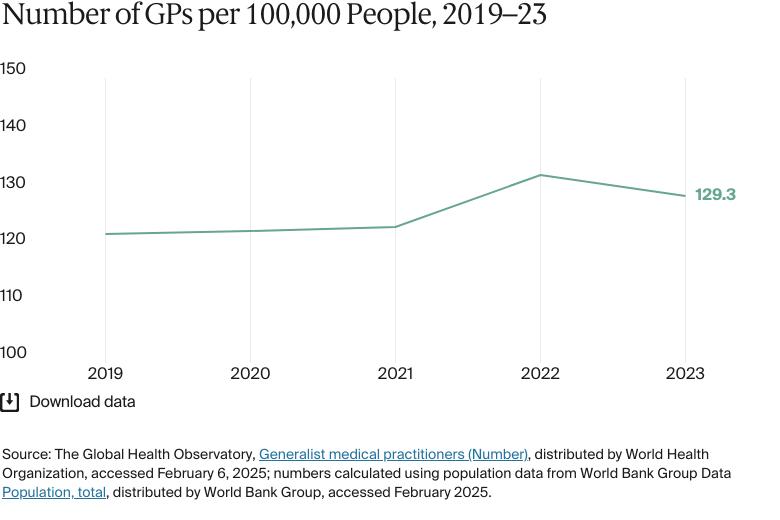
Primary care physicians: 129.3 per 100,000 people
Specialist physicians: 147 per 100,000 people
In 2022, government spending accounted for 71 percent of total health expenditure, while prepaid private health spending was about 14 percent. Spending on drugs is the second highest cost in the health care system after hospitals.
Pharmaceutical spending: Just under 15% of total health care budget
Out-of-pocket spending: 15.2% of total health care spend
Average life expectancy is relatively high, but socioeconomic inequities affect health outcomes.
Adults with low incomes are more likely to have experienced cost-related barriers to health care access and to have waited longer for necessary health care appointments. The life expectancy gap is about 11 years for Inuit people, 10 years for First Nations people, and five years for Métis people. The physician supply gap between urban and rural areas is relatively high in Canada compared with other countries.
Before World War II, health care in Canada was mainly delivered and funded privately. Following the introduction of a universal hospital care plan for all residents in the province of Saskatchewan in 1947, similar plans were created in British Columbia and Alberta by the beginning of the 1950s.1
Between 1957 and 1966, the federal government passed two acts committing to reimburse provinces and territories for half the costs of hospital and diagnostic services (the Hospital Insurance and Diagnostic Services Act [Loi sur l’assurance-hospitalisation et les services diagnostiques]) and non-hospital doctor services (the Medical Care Act [Loi sur les soins médicaux]).2 This legislation is now consolidated under the Canada Health Act of 1984, which describes the goal of health care policy as being “to protect, promote and restore the physical and mental well-being of residents of Canada and to facilitate reasonable access to health services without financial or other barriers.”3
The Canada Health Act also sets out the conditions that provincial and territorial health insurance plans must satisfy to be eligible for federal contributions to health care costs. These contributions are also known as the Canada Health Transfer (Transfert canadien en matière de santé). One condition is that patients should not incur charges to access insured health care services. If they are charged any fees as a condition of receiving care, the province receives a lower Canada Health Transfer.4
In keeping with Canada’s devolved status, administration and service delivery in the health system are decentralized and managed by provincial and territorial governments. According to Amélie Quesnel-Vallée, Canada research chair in policies and health inequalities at McGill University and director of the McGill Observatory on Health and Social Services Reforms (Observatoire McGill sur les réformes de la santé et des services sociaux), this means there can be substantial variations in how and what care is delivered.
The Role of Public Health Insurance
Canada provides universal health care through Medicare, which covers all medically necessary health services for Canadian citizens and permanent residents. Medically necessary services are not defined in the Canada Health Act but are determined by provincial and territorial health care insurance plans in consultation with physician colleges or groups. If these groups deem a service medically necessary, the full cost must be covered by the public health care insurance plan at no cost to the patient.
Residency in a province or territory is the fundamental requirement for obtaining public health insurance coverage. Each province and territory establishes its own minimum residence requirements to determine whether an individual is eligible for benefits under its health insurance plan.5
Non-Canadian holders of employment visas for less than 12 months, foreign students with short-term visas, transient and seasonal workers, refugees, and individuals holding temporary residence permits are not covered by any federal, provincial, or territorial programs.6
Any eligible individual can apply for public health insurance within their province or territory and receive a health card that entitles them to non-emergency health services at public medical facilities.7
Services Covered by Public Health Insurance
Across all provinces and territories, the services that are covered under public health insurance include:8
Preventive care
Inpatient care
Outpatient care
Maternity care
Primary care.
Services with coverage that depends on the province or territory include:
Eye care
Pharmaceuticals
Palliative care
Rehabilitative care
Home visits
Assistive devices
Mental health care provided by a physician.
Safety Nets
Prescription costs are often not fully covered by public health insurance, so most provinces have introduced drug benefit plans for eligible groups to avoid catastrophic spending. Nova Scotia, for instance, has a range of Pharmacare Programs (régime d’assurance médicaments) that help to cover drug costs for groups such as those over age 65, patients with cancer who have low incomes, and patients entering end-of-life care at home.9
At the federal level, the government provides prescription drug coverage for about 1 million people in eligible groups. These include:10
First Nations and Inuit people
Eligible members of the Canadian Armed Forces
Qualified veterans, according to Veterans Affairs Canada
Members of the Royal Canadian Mounted Police
Offenders in federal correctional facilities.
Safety nets for other medical services are usually governed by provinces. In Alberta, for instance, people with permanent medical conditions that prevent them from working are entitled to financial assistance for dental, optical, and diabetes care under the Assured Income for the Severely Handicapped program (Assurance du revenu des personnes sévèrement handicapées).11
Nonprofit organizations provide further support for people with low incomes. For example, the charity Hope Air provides free flights to patients who cannot afford travel costs for medical care — particularly for those living in rural areas.12
The Role of Private Health Insurance
Despite all Canadian citizens having access to Medicare, nearly 70 percent also have private insurance.13 In 2022, the vast majority (90%) of private health insurance plans were group policies purchased by employers; individual policies made up the remaining 10 percent.14 Citizens use private health insurance to supplement gaps in Medicare coverage, which can include:15
Prescription drugs
Eye care
Dental care
Mental health care
Physiotherapy
Chiropractic services.
Private health insurance is prohibited from covering services included in public health insurance.16 This means that private health care services don’t free up any capacity in the public system.
The Role of Government
The provincial and territorial governments are responsible for the management, organization, and delivery of health care services for their residents.
Supported by a portfolio of agencies, the federal government is responsible for:17
Setting and administering national standards for the health care system through the Canada Health Act
Providing funding support for provincial and territorial health care services through the Canada Health Transfer
Directly providing health care services to groups such as First Nations people living on reserves, Inuit people, and serving members of the armed forces
Regulating health products, such as pharmaceuticals and medical devices
Supporting health research, as well as disease monitoring and prevention
Providing tax support (such as credits for disability, medical expenses, and caregivers).
Health Canada (Santé Canada) is the government body responsible for developing national health policy, reducing health inequities, and educating residents about health.18 It also acts as the regulator of pharmaceuticals and medical devices.19
The Public Health Agency of Canada (Agence de la santé publique du Canada) focuses on preventing and managing infectious disease outbreaks, chronic diseases, and injuries and responding to emergency public health threats.20
Integration and Care Coordination
Canada’s decentralized health care system has made it difficult to coordinate care across regions and providers. But the government recognizes that this is important: in October 2023, it announced that it would invest CAD 26.6 million (USD 19.5 million) through the Canadian Institutes of Health Research (Instituts de recherche en santé du Canada) into initiatives designed to advance integrated care, including research into digital solutions and improvements in transitions from hospital to home care.21
There are also plans to increase the use of technology to integrate care. In June 2024, the government introduced the Connected Care for Canadians Act (Loi sur les soins connectés pour les Canadiens) to modernize the health care system. The legislation requires all digital service providers to align on common standards and facilitate secure information exchange across platforms. The government hopes this will enable different health care providers to share health data more easily, reducing treatment delays and the duplication of consultations and tests.22
The provinces are also taking action through programs such as Ontario Health Teams (Équipes Santé Ontario), which aim to connect and integrate health care systems by bringing health care providers together to work collaboratively. Early results indicate that this improves care coordination and patient outcomes.23
Operations and Resources
Overview of the Delivery System
The health care delivery system can be broadly categorized into the following groups:
Primary care includes routine care and care for urgent but minor health problems, including maternity and child care, psychosocial services, liaison with home care, health promotion, and disease prevention. Primary care is typically provided by family doctors — the main term for Canadian primary care providers (GPs) following the introduction of mandatory postgraduate training that changed the terminology — or advanced nurse practitioners.24
Secondary care includes specialist care, such as diagnostic testing and minor surgeries, that are provided in hospitals or specialized clinics. Patients are usually referred to secondary care by family doctors.
Tertiary care includes the treatment of complex and rare conditions, usually provided in tertiary care centers or research hospitals by highly specialized physicians.
Physicians are mainly compensated through fee-for-service models, but for family doctors, this is gradually shifting to alternative models, such as pay-for-performance, group-based profit sharing, and capitation systems. For example, incentive-based bonuses have been used to encourage family doctors to work in rural communities and provide out-of-hours care.25
Primary Care
Primary care is usually a patient’s first point of contact in the health care system. While it is not compulsory for residents to register with a family doctor, many patients choose to do so. This means that they can see the same physician every time and schedule appointments in advance.26
Primary care facilities vary slightly by province and territory, but all include some type of primary care clinic and walk-in center.27 There’s no obligation for primary care clinics to provide out-of-hours services, which means that emergency rooms in rural and urban areas are often used for nonurgent care.28
In 2023, there were 282 medical doctors for every 100,000 people, lower than the average of 360 across other high-income countries.29 There are no data available for the proportion of doctors who are employed privately versus publicly.
Outpatient/Specialist Care
In most provinces and territories, patients need a referral from a family doctor to see a specialist, but they do have some choice in which specialist they’re referred to. There were about 147 specialists for every 100,000 people in 2023.30 There are no data available for the proportion of specialists employed privately versus publicly.
Specialists are mainly paid on a fee-for-service basis. Most specialists bill provincial and territorial governments directly for their services, but some are salaried employees of hospitals and other health care facilities.31
Physician Education and the Workforce
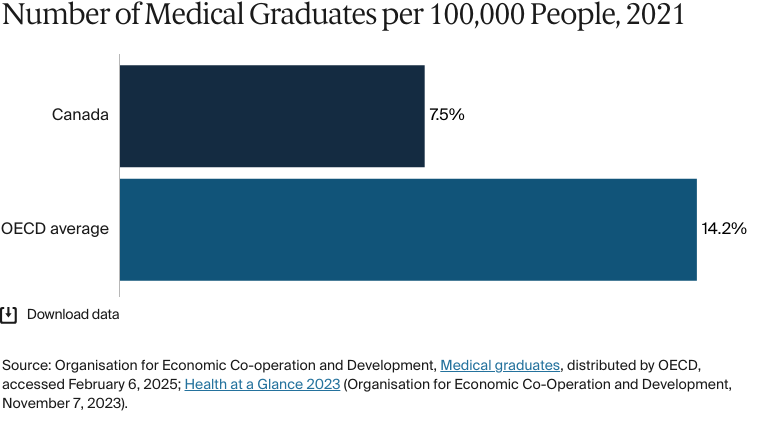
There were 7.5 medical graduates for every 100,000 people in 2021, decreasing to 7.3 in 2022, one of the lowest rates among Organisation for Economic Co-operation and Development (OECD) countries.32 Students enrolled in one of the 17 public medical schools paid an average annual tuition fee of CAD 16,039 (USD 11,783) for the 2024–25 academic year.33 Many physicians receive their medical education abroad — in 2022, 27 percent were international graduates.34
According to Quesnel-Vallée from the McGill Observatory on Health and Social Services Reforms, strict regulation of the number of physicians trained annually limits the size of the health workforce. “We deliver a very limited number of practice permits, and that is restricting the number of physicians to one of the lowest per capita ratios in high-income countries,” says Quesnel-Vallée. “But physicians are only the beginning because you also need other health professionals. And we also have shortages of nurses and other technicians.”
The location of medical professionals also affects access to care because the population is highly dispersed. In 2022, just 7 percent of physicians were based in rural communities, with the remaining 93 percent working in urban areas.35 To reduce doctor and nurse shortages in rural areas, the federal government offers student loan repayment assistance to health care workers in underserved regions.36
In 2023–24, the average annual salary for a physician was CAD 383,000 (USD 271,085). Family doctors received an average of CAD 324,000 (USD 226,271), while medical specialists received an average of CAD 406,000 (USD 289,451).37
Hospitals
BY THE NUMBERS
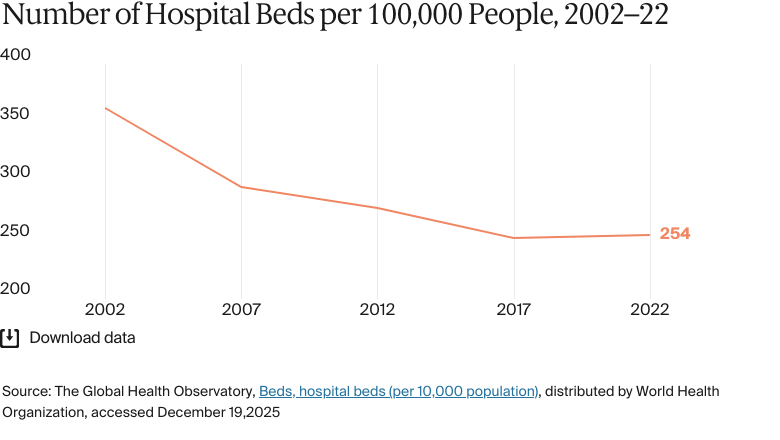
In 2022, there were 254 hospital beds per 100,000 people.38
In 2023, there were 1,126 nurses per 100,000 people (compared with an average of 1,052 across high-income countries in 2022).39
Most hospitals are funded through global budgets, either directly by ministries of health or indirectly via budget allocations to provincial or regional health authorities. In hospitals that contract with health authorities, such as the ones in Ontario and Catholic hospitals in Western Canada, funding is generally based on the previous year’s allocation, adjusted for inflation and budget growth.40
Some jurisdictions have been exploring alternative funding mechanisms, including activity-based funding. Most non-physician health care personnel, including regulated nurses — the largest group — are salaried employees within health organizations.
The proportion of hospital beds for every 100,000 people has decreased over the past two decades as the population has increased. In 2000, there were 375 beds for every 100,000 people; in 2022, there were 254 for every 100,000 people.41 At the same time, occupancy rates are rising. Canada is one of only three OECD countries with an occupancy rate above 85 percent.42
Mental Health Care
BY THE NUMBERS
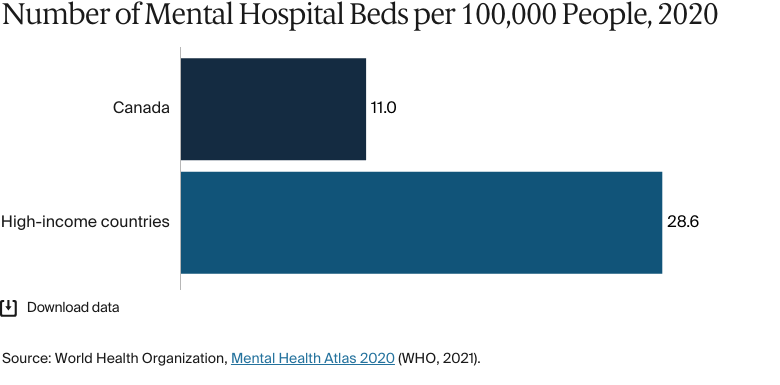
In 2020, there were 11 mental hospital beds per 100,000 people, compared with 29 across all high-income countries.
There were 14 psychiatrists per 100,000 people in 2020, higher than the average of nine for high-income countries.
In 2020, there were 283 mental health professionals per 100,000 people, much higher than the average of 62 in high-income countries.43
Proportionally, there are many more mental health professionals in Canada than in other high-income countries. But not all mental health services are covered by public health insurance.
As with all health care, psychiatric services deemed medically necessary are covered by the public system. There’s limited support available from social workers and clinical counselors through government-funded hospitals, clinics, and employee assistance programs. Community-based services and not-for-profit agencies, such as peer support groups and the Canadian Mental Health Association (Association canadienne pour la santé mentale), provide additional assistance.
The federal government has invested in several mental health care programs, including Togetherall, which provides care for students, young adults, and teens, and the Hope for Wellness Help Line, which provides care for Indigenous people.44
For services not covered by public health insurance or alternative programs, individuals either rely on private insurance, often provided by employers, or pay out of pocket.
Long-Term Care and Social Support
Long-term, facility-based care is excluded from public insurance under the Canada Health Act. Long-term care services are mainly administered by provinces, territories, and municipalities, with the federal government providing funding through transfer payments for health and social services. Funding allocation for long-term care shows that 87 percent is spent on residential care, and 13 percent is allocated to home and community care.45
In 2020, most elderly residents (about 92%) lived in private dwellings in communities. About 7.9 percent lived in residential care facilities.46
Residential long-term care is expensive, up to CAD 8,000 (USD 5,877) per month in some provinces. Government subsidies are limited, so some people choose to purchase long-term care insurance. These policies offer coverage for patients suffering from chronic illness; disability; cognitive impairment, such as dementia; and age-related conditions. Patients can use this insurance to cover residential care in nursing homes or chronic care facilities or home care services.47
In April 2021, the Canadian Institute for Health Information (Institut canadien d’information sur la santé) reported that 46 percent of long-term residential care homes are publicly owned.48
Cost and Affordability
Health Care Spending Overview
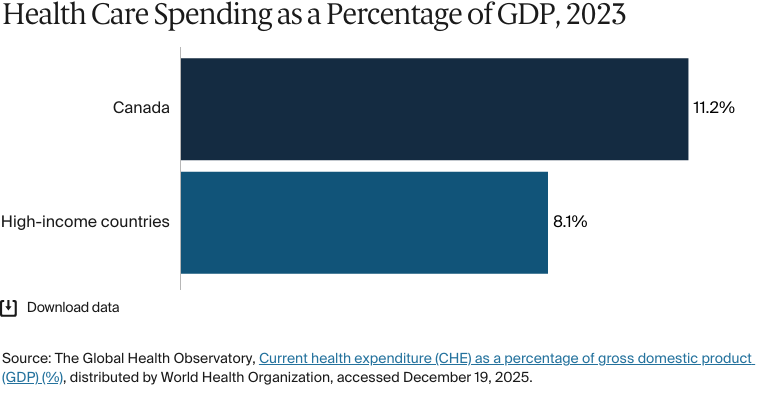
Canada spent 11.2 percent of gross domestic product (GDP) on health care in 2023, compared with an average of 8.1 percent in high-income countries.49 In 2022, government spending accounted for 71 percent of total health expenditure, while prepaid private health spending was about 14 percent.50 In 2023, out-of-pocket spending was 15.2 percent of total expenditure.51
We ensure equitable access through the removal of any user fees or copayments for essential hospital and physician services, but we have major gaps in coverage, where we see a lot of inequities for financial reasons. For sectors such as prescription drugs and dental care, we rely heavily on private insurance and out-of-pocket payments.
Sara Allin
Associate Professor of Health Policy
Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health, University of Toronto
Pharmaceutical Spending
Hospitals dispense drugs free of charge to inpatients as part of Medicare. Outpatients receive prescriptions from physicians and occasionally from other health providers authorized to prescribe certain classes of drugs. These prescriptions may be covered in whole or in part by public and private pharmaceutical plans. Provincial and territorial governments manage drug plans for their residents, stipulate which people will be covered by public plans, and determine the extent of that coverage.52
Spending on drugs is the second highest cost in the health care system after hospitals.53 In 2023, just under 15 percent of total health spending was on pharmaceuticals, with an average spend for every person of CAD 1,223 (USD 1,035).54 Drug prices are about 25 percent above the OECD median, which affects the sustainability of the health care system.55
Health Canada collaborates with provinces and territories through the pan-Canadian Pharmaceutical Alliance (pCPA; Alliance pharmaceutique pancanadienne). This collaboration allows Health Canada to use collective buying power to reduce drug costs, including generic drug prices, and to modernize regulations on patented drug prices to protect consumers from high costs.56
Cost Sharing and Out-of-Pocket Spending
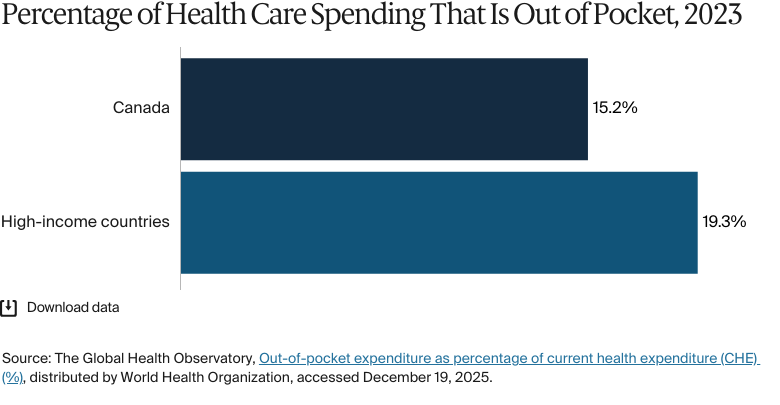
The Canada Health Act and corresponding provincial and territorial legislation have largely eliminated user fees and patient charges for hospital and physician services, but many other health care services still involve direct charges to patients. In 2023, out-of-pocket payments accounted for 15.2 percent of total health spending, compared with an average of 19.3 percent in high-income countries.57 The majority of these expenses were directed toward dental care, prescription drugs, and long-term care services.58
Supplemental private insurance plans often include deductibles, copayments, and coinsurance for services such as vision, dental care, and other health services provided by physiotherapists, psychologists, dietitians, and occupational therapists. Provincial drug plans to cover prescriptions also have deductibles and copayments.59
Copayments for non-insured health services can vary. For example, several provinces, including British Columbia, Ontario, and Quebec, have means-tested deductibles.60
There are no data available for the percentage of the population that is pushed below the poverty line by health care costs.
How Are Costs Contained?
The federal Patented Medicine Prices Review Board (Conseil d’examen du prix des médicaments brevetés) is an independent body that regulates the introductory prices of new patented medications at the manufacturer level. But it doesn’t regulate wholesale or pharmacy prices, nor does it have authority over pharmacists’ professional fees.61
The pCPA aims to use the combined negotiating power of participating jurisdictions to get better value for publicly funded drug programs and patients. As of April 2025, collective negotiations by the pCPA had achieved annual savings of CAD 3.9 billion (USD 2.7 billion) from brand-name drugs and CAD 935 million (USD 654 million) from generic drugs.62
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
The top three causes of death in 2021 were:
Ischemic heart disease: 110 per 100,000 people
Alzheimer’s disease and other forms of dementia: 81 per 100,000 people
Trachea, bronchus, and lung cancers: 53 per 100,000 people.63
The maternal mortality rate was 12 deaths per 100,000 live births in 2023 (compared with 12 on average in high-income countries).64
The avoidable mortality rate was 184 deaths per 100,000 people in 2022.65
The infant mortality rate was 440 deaths per 100,000 live births in 2023 (compared with 410 on average across high-income countries).66
In 2021, the share of the population with mental health disorders was 15 percent (compared with 16% on average in high-income countries).67
The suicide rate was 12 deaths per 100,000 people in 2023.68
Homelessness affected 100 people per 100,000 in 2022.69
Guns were responsible for three in every 100,000 deaths in Canada in 2023.70
26 percent of adults were affected by obesity in 2022.71
Average life expectancy was 81.6 years in 2021, slightly higher than the average for high-income countries (79.7 years). Women live about four years longer than men (83.8 years compared with 79.4 years).72
Average life expectancy is relatively high, but socioeconomic inequities affect health outcomes. Adults with low incomes are more likely to have experienced cost-related barriers to health care access and to have waited longer for necessary health care appointments.73
There are gaps in outcomes between Indigenous and non-Indigenous people. The life expectancy gap is about 11 years for Inuit people, 10 years for First Nations people, and five years for Métis people.74
There are also geographical barriers to accessing health care. The physician supply gap between urban and rural areas is relatively high in Canada compared with other countries. In particular, people in northern provinces are more likely to have difficulty accessing care.75
Addressing Health Inequities
The government is taking steps to understand and address health inequities between different populations. The pan-Canadian Health Inequalities Reporting initiative (L’initiative pancanadienne sur les inégalités en santé), for instance, was established to improve the measurement, monitoring, and reporting of health inequities to inform policymaking.76
To address the shortage of physicians in rural areas, provinces have introduced their own programs as additions to federal incentives (see Physician Education and the Workforce). For example, Ontario’s Northern and Rural Recruitment and Retention Initiative (Initiative de recrutement et de maintien des effectifs dans le Nord et en milieu rural) offers relocation grants, education subsidies, and enhanced compensation to physicians practicing in underserved communities.77 Alberta’s Rural Remote Northern Program, meanwhile, offers two compensation methods to physicians working in underserved areas: a flat fee payment for physicians living and delivering services in eligible communities and a variable fee premium automatically applied to physicians providing services in eligible communities — regardless of residency.78
Indigenous Services Canada (Services aux Autochtones Canada) collaborates with partners to enhance access to high-quality services for Indigenous peoples. It does this through a mix of dedicated health care services (including mental health and family health), education, and funding support.79 The Non-Insured Health Benefits Program (Programme des services de santé non assurés) is an important part of this, providing eligible First Nations people and Inuit people with coverage for vision care, dental care, counseling, medical supplies, prescriptions, and medically necessary transportation.80
Innovation and Reform
Health Care Innovation
Canada has introduced several major innovations and reforms to improve the quality of its health care. The federal government has committed nearly CAD 200 billion (USD 147 million) over 10 years with the aim of improving access to primary care, reducing wait times, and enhancing mental health services. Within this funding, CAD 25 billion (USD 17.5 billion) has been allocated to specific programs within provinces and territories to address their particular needs.81
The introduction of the Pharmacare Act (Loi concernant l’assurance-médicaments) in 2024 provided increased coverage for a number of contraceptive drugs and diabetes medications. This is the first phase of the government’s plans for universal coverage for essential drugs.82
Canadian health care reforms have emphasized the adoption of team-based primary care to address the shortage of family doctors and improve access to services. These teams can include family doctors, nurse practitioners, pharmacists, psychologists, psychotherapists, and dieticians, who work together to provide patients with timely access to tailored care.83 The Canadian Medical Association (Association médicale canadienne) is advocating for these primary care teams to be available to 50 percent of Canadians within five years and 80 percent within 10 years.84
Health Care Technology
Electronic Health Records
Canada Health Infoway (Inforoute Santé du Canada) is a government-funded nonprofit that focuses on developing and adopting electronic health records (EHRs). The use of EHRs has risen: in 2015, 73 percent of family doctors used them, and in 2022, 93 percent used them.85
But according to a national survey, fewer than 40 percent of Canadians (excluding those in Quebec) have accessed their health information online. In February 2023, the government, provinces, and territories agreed that one of their shared health priorities must be to allow people online access to their health information.86
The Public Health Agency of Canada is collaborating with the Canadian Primary Care Sentinel Surveillance Network (Réseau canadien de surveillance sentinelle en soins primaires) to access primary care EHR data. Using these large data sets, the Public Health Agency of Canada can identify patterns that might not be visible in smaller data sets, with the aim of improving risk assessment and trend analysis in priority areas.87
E-Prescriptions
Canada Health Infoway has also established the country’s national e-prescription service, PrescribeIT®, which allows clinicians to send prescriptions directly from their EHRs to pharmacies. The service is designed to improve efficiency and patient safety and eliminate the need to fax paper prescriptions.88
Artificial Intelligence
In the field of radiology, artificial intelligence (AI) has been widely deployed to improve diagnostic accuracy and efficiency. And the Canadian Agency for Drugs and Technologies in Health (Agence canadienne des médicaments et des technologies de la santé) has published reports on AI applications in cancer diagnostics to investigate the technology’s potential to improve cancer care. More broadly, machine learning is being employed to improve diagnostic accuracy and treatment planning.89
AI is also being used to improve the efficiency of patient contact centers. Patient contact centers are digital platforms that track and manage patient interactions with health care systems, such as emails, phone calls, and online chats. A new project called the CareAI Initiative has secured CAD 44 million (USD 32 million) to automate routine tasks, reduce data entry errors, liaise with patients, and streamline workflows for medical professionals.90
Telemedicine
Canada is accelerating the use of mobile health apps and wearable technologies for conditions such as diabetes and cardiovascular diseases. Telehealth is also being used to treat and manage mental health conditions. For example, Ontario offers a variety of apps and digital tools to its residents.91 Some provinces and local governments have also introduced teleassistance initiatives to provide remote support to those not living in residential care.92
But the use of telehealth is sporadic. According to Sara Allin, “[There are] examples of innovation everywhere: at the provider, hospital, and clinic [levels]. But these aren’t supported by any central or harmonized data systems, which would enable us to scale up these pilots or programs. There’s huge potential, but change in Canada is very rare, so we’re a little stuck.”
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
“Urgent action needed to protect seniors in long-term care,” Canadian Association of Retired Persons (Association canadienne des personnes retraitées), accessed December 4, 2025, https://www.carp.ca/longtermcare/.
↩
Institute for Health Metrics and Evaluation, GBD compare, distributed by IHME, accessed December 4, 2025, https://vizhub.healthdata.org/gbd-compare/; overall firearm mortality is the aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
71
World Health Organization, Age-standardized prevalence of obesity among adults (18+ years), distributed by WHO Data, last updated February 29, 2024, https://data.who.int/indicators/i/C6262EC/BEFA58B.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.