Denmark’s health care system provides coverage for all legal residents. Services are mainly funded through general taxation and administered at the regional and municipal levels. All residents are entitled to essential hospital and physician services without paying out of pocket, but nearly half of the population purchases voluntary health insurance to help cover dental care and prescription drugs.
Denmark performs well on several health indicators, including life expectancy, which is above the average for high-income countries.1 The country also spends a comparatively lower share of its gross domestic product on health care, and out-of-pocket costs remain relatively low.2 Despite these strengths, the health system faces several challenges, including ensuring coordination across a decentralized framework, addressing workforce shortages, and reducing wait times for treatment.3
Denmark has a well-established tradition of public welfare provision. While there is no formal public health insurance program in Denmark, all registered residents can access comprehensive health care services free of charge. Under Strukturreformen, the last significant federal reform, regions and municipalities took on a leading role in implementing changes to health services and launching local policy initiatives to meet residents’ needs.
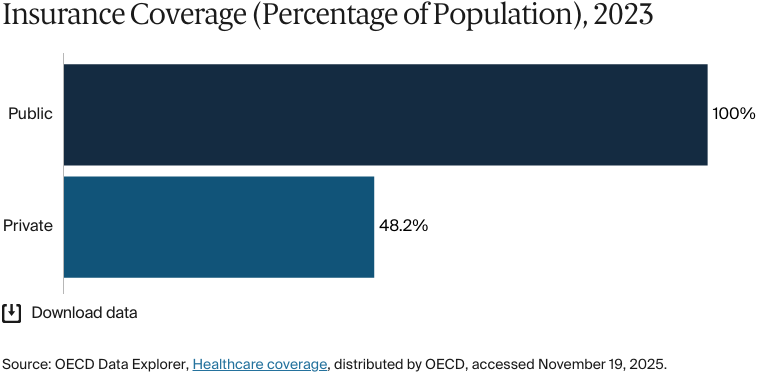
Public insurance coverage: 100% of population
Private insurance coverage: 48% of population
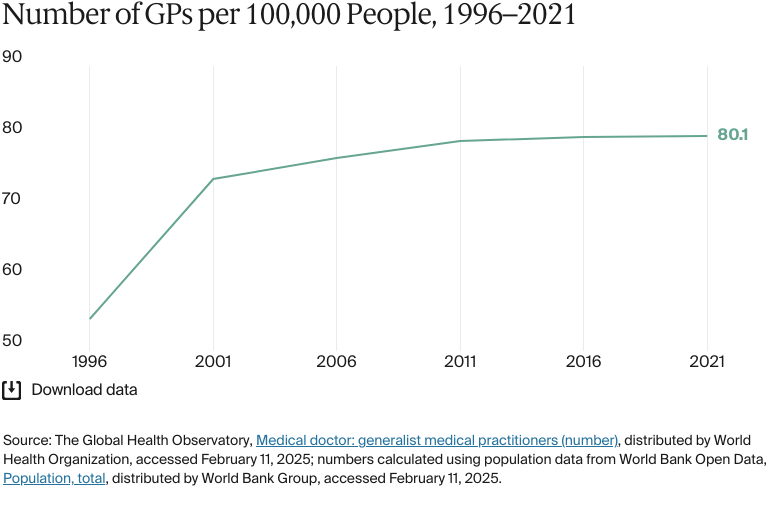
Primary care physicians: 80.1 per 100,000 people
Specialist physicians: 193.5 per 100,000 people
Total health care expenditure was DKK 278 billion (USD 44 billion) in 2024. Government spending accounts for most of total health expenditure (84.6%). Health care in Denmark is mainly funded by general taxation.
Pharmaceutical spending: 7.5% of total health care budget
Out of pocket spending: 13% of total health care spend
Individuals with only primary-level education experience higher rates of illness, worse health outcomes, and shorter lifespans than people with tertiary education.
Ethnic minorities have higher rates of preterm births and cesarean sections and are less likely to participate in vaccination programs and routine child health checks. Migrant adults also encounter barriers to accessing primary care and dental services and rely more on emergency services.
Denmark has a well-established tradition of public welfare provision. In 1970, an administrative reform established the structure of the health care system, assigning responsibility for hospitals to 14 counties and establishing general taxation as the primary funding source.4
Further legislation in 1993 granted patients the freedom to choose among public hospitals. This policy was later expanded to allow patients who had waited over two months for diagnosis or treatment at a public hospital to receive services at a private hospital or a facility abroad, with full coverage.5
In 2007, a major administrative reform, the Local Government Reform (Strukturreformen), replaced 14 counties with five regions, which assumed responsibility for hospital and outpatient care, general practitioners (GPs), and private practice specialists. The reform also consolidated Denmark’s municipalities from 275 to 98 and gave them responsibility for rehabilitation, disease prevention, disability care, and substance abuse treatment.6
Under Strukturreformen, the last significant federal reform, regions and municipalities took on a leading role in implementing changes to health services and launching local policy initiatives to meet residents’ needs.7
The Role of Public Health Insurance
While there is no formal public health insurance program in Denmark, all registered residents can access comprehensive health care services free of charge. Nonresidents and undocumented migrants are automatically entitled to emergency care but not elective care.8 Asylum seekers are entitled to necessary care — funded by the Danish Immigration Service — that covers urgent treatment needed to prevent a life-threatening injury, the serious worsening of a condition, or a condition from becoming chronic.9
Residents can choose between two coverage options: group 1 provides free access to specialists after a referral from a GP, and group 2 provides direct access to specialists without the need for a referral, but patients are subject to copayments. Nearly all residents (99%) choose group 1, while only 1 percent choose group 2.10
Services Covered by Public Health Insurance
Residents can access the following free of charge:11
Preventive care
Inpatient care
Outpatient care
Maternity care
Primary care
Pharmaceuticals (covered if prescribed in hospitals; otherwise, requires a copayment)
Dental care (free for people age 22 and under, with other patients subject to copayments of 35 to 60%)
Eye care (basic eye exams and treatments)
Mental health care
Palliative care
Rehabilitative care (may require a copayment)
Home visits
Assistive devices (provided by the municipality or subsidized).12
Long-term care coverage is means-tested and usually requires a copayment.13
Safety Nets
Inpatient prescriptions are covered for all residents, and prescription drugs for outpatients are subsidized. Residents also incur copayments for medicines prescribed by a GP or a practicing specialist. Municipalities pay for or subsidize prescribed medical devices.14
Over the past two years, Denmark has broadened free access to comprehensive dental care for anyone under age 22. Regions also subsidize dental care for older adults, particularly preventive services.15 Copayments vary depending on individual patient circumstances and the region.16
If a GP refers a patient for outpatient physiotherapy or psychological therapy, care is often subsidized. Chiropractic care is subsidized and doesn’t need a GP referral.17
The Role of Private Health Insurance
In 2023, about 48 percent of the population purchased voluntary private health insurance, which mainly covers copayments and reimbursements for private health care, such as dental care and outpatient prescriptions.18
About 32 percent of residents have supplementary insurance for expanded access to private providers. These programs are typically provided through annual or long-term contracts and pay benefits in cash. About 90 percent of people with supplementary insurance receive this through their employers.19
The Role of Government
Denmark’s health system is organized into three administrative levels: federal, regional, and municipal. The federal government provides the overall framework, including guidelines, standards, policy initiatives, and regulations for health care organizations and professionals. The regions and municipalities plan and provide health care services.20
Providing hospital, physical, and psychiatric care
Paying private practitioners, such as GPs, specialists, dentists, physiotherapists, and chiropractors, for public sector work
Regulating the number of private practitioners who can be reimbursed from the public system
Paying private clinics to treat patients, according to contracts or wait time guarantee requirements.
Municipalities finance and provide:
Public health and health promotion
Some dental services
Health visitors
School health services
Substance abuse treatment
Home help and home nurses
Nursing home care
General rehabilitation.
An annual financial agreement between the state, regions, and municipalities sets overall budgets and municipal taxes, including the level of state subsidies.
Integration and Care Coordination
Every four-year election cycle, regions and municipalities form health care agreements to align their activities, resources, and referral processes. Representatives from the regions and municipalities, as well as private practitioners, form regional consultative committees that monitor progress against these agreements, but they’re not legally binding.22
Other examples of efforts to improve collaboration and integration include the following:
The Health Structure Commission was created in 2023 as a government-instructed body tasked with reviewing the structure of Denmark’s health care system and suggesting reforms to improve coherence.
The creation of 21 health clusters, each with an emergency hospital at its center, aims to integrate services provided by hospitals, municipalities, and general practices, including psychiatric services. The clusters include joint administrative and political committees that promote closer collaboration, better coordination of health care delivery across sectors, improved continuity of care, and more cohesive patient care pathways.
A national strategy for chronic disease management has been developed, focusing on care, patient education, and services.23
“The big challenge is how to work closely together and ensure a coherent and well-coordinated pathway where the patient has a good experience from the very beginning to the very end,” says Mette Maria Skjøth, chief administrative officer at Odense University Hospital.
The fundamental principle of the Danish health care system is that every person should be treated with respect and autonomy, and that the health care system should fulfill the needs of the population with respect to easy and equal access. That requires attention, collaboration, and appropriate structures.
Mette Maria Skjøth
Chief Administrative Officer
Odense University Hospital
Operations and Resources
Overview of the Delivery System
Primary care: GPs are patients’ first point of contact. They provide routine care, manage common illnesses, and coordinate referrals to specialists.
Secondary care: Hospitals provide specialized medical services, such as advanced diagnostics, treatments, and surgeries. These often require a GP referral to a specialist.
Tertiary care: Specialized hospitals and centers provide advanced treatments for complex and rare medical conditions.
Patients in group 1 (see The Role of Public Health Insurance)don’t pay out of pocket for primary or specialist care consultations and treatments. However, group 2 patients incur copayments to access specialists without a GP referral.
Hospitals are mainly funded through prospective global budgets and performance-based financing, usually based on care continuity.24 GPs are paid via a mix of weighted capitation and fee-for-service payments. Specialists and dentists are paid on a fee-for-service basis and negotiate their fees with regional authorities.25
Primary Care
Residents must register with a GP. These physicians handle 90 percent of all medical cases.26
GPs are self-employed and work as solo practitioners or in GP cooperatives — large-scale groups of GPs who are supported by additional personnel. The collaborative approach has become more common, with the proportion of cooperative practices increasing from 27 percent of general practices in 1977 to 59 percent in 2022.27 In the North, Central and Southern regions of Denmark, GP cooperatives provide out-of-hours care from late afternoon until 11pm, with services including GP-led telephone triage, telephone advice, face-to-face consultations, and home visits.28
GPs work under a national agreement on tariffs and follow regional plans that outline capacity and focus areas.29 Their income is a mix of capitation (based on patient lists) and fee-for-service payments.30
In 2021, there were 80.1 GPs for every 100,000 people.31 There are no data available for the proportion of primary care physicians employed privately versus publicly.
Outpatient/Specialist Care
As most residents opt for group 1 coverage (see The Role of Public Health Insurance), patients typically need a referral from their GPs to access services such as specialist consultations and surgery.32
Most specialist care takes place in public hospitals, inpatient clinics, outpatient clinics, or, in some cases, 24-hour emergency wards.33 Doctors and other health professionals are salaried hospital employees. In 2020, there were 193.5 specialist medical practitioners for every 100,000 residents.34
On average, there are fewer outpatient visits in Denmark than in the European Union (E.U.), but the number has substantially increased over the past 20 years. One reason is a shift away from inpatient care, with more treatments and diagnostics being carried out in outpatient clinics. This shift has also caused the average length of hospital stays to decrease.35
Physician Education and the Workforce
The government is responsible for the regulation, supervision, and fiscal management of medical education.36
The four medical schools in Denmark don’t charge tuition fees for Danish students or for international students from the E.U./European Economic Area countries or Switzerland. Students from other countries have to pay between EUR 6,000 (USD 6,280) and EUR 16,000 (USD 16,748) per year, depending on the institution.37
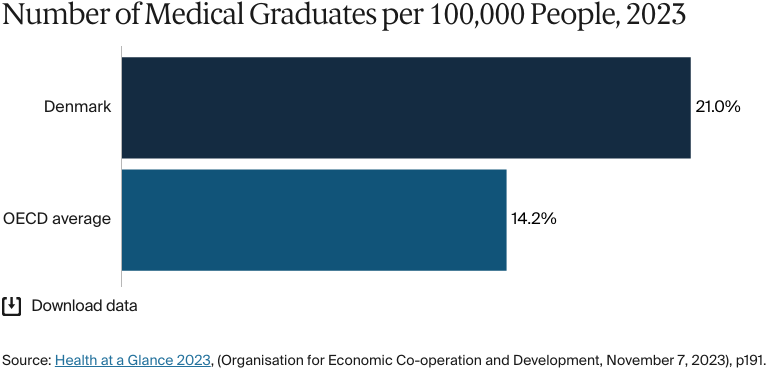
In 2023, there were 21 medical graduates per 100,000 people, slightly below 2021 figures (22) but still significantly higher than the OECD average (14.2).38
New graduates are assigned to one-year positions, divided into two six-month placements in internal medicine, surgery, psychiatry, or general practice. Placements are distributed among specialties and throughout the country based on need and capacity. After completing their basic clinical education, physicians enter specialist training for 48 to 60 months. As with their initial training, candidates are placed in multiple departments and hospitals.39
There are shortages of doctors in specialties such as psychiatry, radiology, and general practice, especially outside the major cities. The government is trying to address these shortages with short-term measures to reduce wait times, alongside long-term strategies. In 2022, the government agreed on a new health reform package to increase the number of GP training positions and created a resilience commission (Resilienskommissionen) to address other shortages.40 The resilience commission provided 20 recommendations under three core themes:
Prioritize tasks to reduce workforce requirements more effectively.
Make health care workplaces more attractive and improve long-term retention.
Make the education system more flexible and strengthen the link between workplace requirements and training.41
The 2022 reform also enabled regions to offer a financial subsidy for GP training in areas experiencing shortages. Following these initiatives, the number of GPs is expected to increase by 43 percent between 2022 and 2035.42
Health care providers are also looking at ways to improve the recruitment and retention of medical professionals.
“We try to have attractive career pathways,” says Skjøth. “[At Odense University Hospital], we have a strong focus on workforce development, and […] shift schedules are planned in a fair way. Furthermore, we have a distinct focus on management and leadership to ensure knowledge, support, and well-being for our personnel”.
Hospitals
BY THE NUMBERS
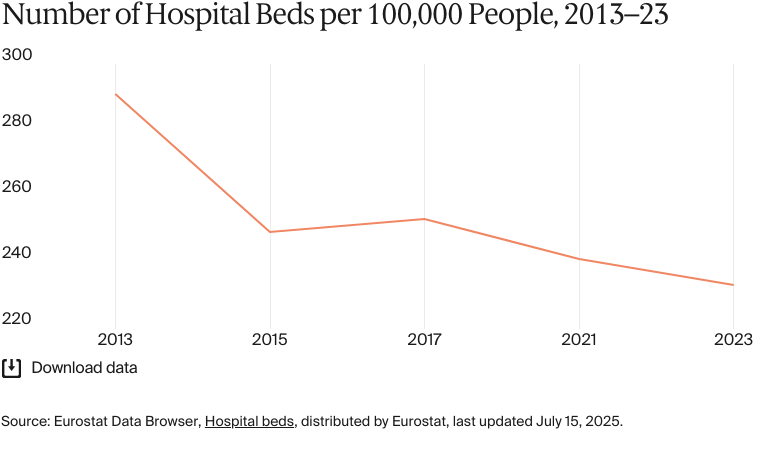
In 2023, there were 233 hospital beds per 100,000 people (compared with an average of 511 across the E.U.).43
In 2021, there were 1,219 nurses per 100,000 people (compared with an average of 826 across Europe in 2022).44
The Danish Health Authority (Sundhedsstyrelsen) oversees the overall distribution and planning of specialized hospital services to improve uniformity and quality across the health care system.45
Denmark introduced prospective global budgets in 1982 to control hospital budget deficits and overall health care costs. Since then, the government has sought to balance cost control with incentives for value-based care.46
In the 1990s, activity-based financing, mainly through diagnosis-related groups, was implemented to allocate hospital budgets based on the number and complexity of treatments.47 The system increased hospital activity but also introduced perverse incentives that led to prioritizing hospital treatments over telemedicine. To redirect focus to patient outcomes and care quality, Denmark has moved gradually to a system that combines activity-based funding with performance measures.48
More than 95 percent of hospital beds are in public hospitals. Each region hosts one or more university hospitals with tertiary care capabilities, as well as district general hospitals. If regions don’t meet wait time guarantees (30 days for diagnosis and an additional 30 days for treatment), they have to arrange treatment at private hospitals or clinics. Regions can also negotiate additional local agreements with private hospitals to increase capacity in particular areas.49
One of the goals of the Strukturreformen reforms was to improve acute services and quality of care, in part by reducing the number of acute hospitals in each region and centralizing specialized care in fewer hospitals. Between 2007 and 2017, hospital productivity rose by more than 2 percent per year, while costs and wait times remained stable. Staff workloads increased, while residents in more remote areas had to travel further to receive specialist or emergency care.50
As hospital numbers decreased, so did the number of beds. In 2023, the number of hospital beds for every 100,000 people dropped to 233, from 253 in 2018.51 Meanwhile, the number of nurses for every 100,000 people increased from 1,202 in 2020 to 1,219 in 2021.52 Denmark plans to invest DKK 4 billion (USD 584.5 million) in 25 local hospitals to improve services in more remote areas and address chronic care needs.53
Mental Health Care
BY THE NUMBERS
In 2022, there were 19 psychiatrists per 100,000 people, compared with 29 across all high-income countries in 2020.54
Multiple entities manage mental health care. As with physical health care, the state regulates the system. Regions handle most inpatient and outpatient services; municipalities deliver social and preventive services, including support for addiction issues; GPs manage mild to moderate conditions; and interdisciplinary teams provide outpatient care. All residents have free access to mental health services, but private psychiatric and psychological care requires out-of-pocket payments.55
Anxiety and depression are the most common mental health issues in Denmark. There are gender and socioeconomic disparities in depression rates: individuals with lower incomes, particularly women, are about three times more likely to report experiencing depression.56
Patients pay out of pocket for at least a portion of private psychiatric and psychological care.57 In 2021, certain groups became eligible for subsidized psychological treatment. The subsidy, which covers 60 percent of the cost, requires a doctor’s referral. The groups that are covered are:
Victims of certain crimes (for example, robbery and rape) and traffic accidents
Relatives of people who have serious mental illnesses
People who are affected by a seriously debilitating illness and their relatives
Next of kin in the case of death
People who have attempted suicide
People who have had an induced abortion after the 12th week of pregnancy
People over age 18 with mild to moderate depression or anxiety.58
The Strukturreformen continued a shift from long-stay psychiatric hospitals to community-based services. In 2022, the government announced a 10-year plan to enhance psychiatry and mental health care, beginning with five priorities:
Expanding accessible municipal services for children and youth with mental health issues
Improving regional psychiatric services for those with severe conditions
Increasing mental health information and combating stigma
Advancing multidisciplinary, evidence-based prevention and treatment
Supporting research into mental disorder prevention and treatment.59
The coalition government that took office in 2022 has committed to prioritizing psychiatry by allocating DKK 4 billion (USD 584 million) annually to funding plans.
There are no data available for the size of the mental health workforce or the number of mental hospital beds.
Long-Term Care and Social Support
Municipalities are responsible for social services, such as sickness allowances, disability pensions, and care for the elderly, people with disabilities, and those with chronic conditions or mental health issues.They’re also responsible for housing people with learning disabilities. However, to improve cost-effectiveness, nonprofit agencies are increasingly handling long-term inpatient care, day care, and other social services.60
Long-term care at home is free, but temporary care can require copayments based on the recipient’s income. Nursing homes and sheltered housing are partly financed by residents, with low-income individuals contributing a portion of their pensions. About 11.6 percent of people age 67 and over lived in care homes in 2023.61
Municipalities help with shopping, housework, and personal hygiene, and help family caregivers in supporting elderly people so they can remain independent at home. Elderly people can also receive services at day-care centers, and a 24-hour phone system gives them access to a public health nurse in case of an emergency. This has proven to be a cost-effective way of caring for the elderly, as it is cheaper than senior residences, gated communities, assisted living units, and nursing homes.62
As with other health care services, there is a shortage of long-term care workers, and an aging population is exacerbating this issue.63
Cost and Affordability
Health Care Spending Overview
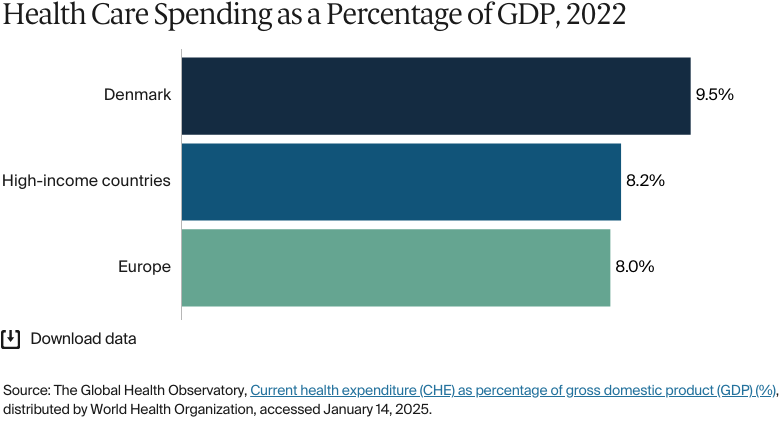
Total health care expenditure was DKK 278 billion (USD 44 billion) in 2024.64In 2022, Denmark spent 9.5 percent of its gross domestic product (GDP) on health care, less than neighboring countries, such as Germany and Sweden, but higher than the European and high-income country averages.65
Government spending accounts for most of total health expenditure (84.6%); out-of-pocket spending accounts for 13.1 percent, and prepaid private spending accounts for 2.3 percent.66
Health care in Denmark is mainly funded by general taxation. The regions receive about 83 percent of their revenues from state block grants, which are allocated based on population size, socioeconomic factors, and demographics. Supplemental funding includes municipal copayments for services provided to local residents and performance-based state financing based on continuity of care.67
Municipalities are funded by proportional income and land taxes and block grants from the state. As with the regions, the block grants are distributed according to population size and socioeconomic status. The funds are then redistributed among the municipalities to equalize disparities in expenditure needs and taxation bases.
Pharmaceutical Spending
Denmark’s pharmaceutical spending per capita is about USD 495 per year, lower than that of the U.S., Germany, and Sweden. Denmark also spends less on pharmaceuticals than those countries, in terms of the share of total health spending (only about 7.5%).68
While medications prescribed in hospital and some outpatient hospital treatments are free, medications prescribed by GPs or private specialists usually requires out-of-pocket payment.69
Cost Sharing and Out-of-Pocket Spending
Patients typically pay out of pocket for dental care, physiotherapy, chiropractic care, and psychiatric services provided outside hospitals.70
For dental care, the reimbursable amount depends on the procedure. Usually, only a smaller part of the total cost is covered, leading to high out-of-pocket payments. Dentistry is an area where copayments are not limited.
Copayments for reimbursable prescription medicines generally depend on the individual’s total annual spending on these medications. Nationally, the maximum annual copayment for reimbursed prescription medicines is DKK 4,735 (USD 687) in 2025.71
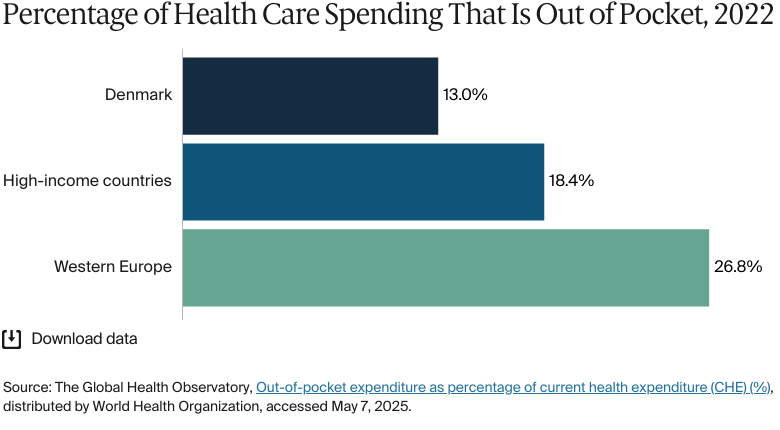
Household out-of-pocket payments accounted for 13 percent of total health expenditure in 2022, compared with 18.4 percent for high-income countries.72 Free universal coverage means that no resident is pushed below the poverty line as a result of health care costs.73
How Are Costs Contained?
Health care costs are contained through global budgets for regions and municipalities, collective purchasing of generic pharmaceuticals, and incentives to transition care from inpatient to outpatient settings.74
Other efforts include value-based health care models, which focus on patient outcomes rather than the volume of services provided. Integrated care models also encourage collaboration among primary care providers, specialists, and hospitals, which can reduce fragmentation and duplication of services.
In 2023, the Danish government and the Danish regions signed an agreement to reduce the price the public sector pays for patients to be treated at private hospitals and clinics. A 10 percent price drop for private care was in place until June 2025. The agreement also allowed private hospitals to offer more specialized treatments for areas with particularly long wait lists. Before this, the private sector was forbidden from providing these services.75
Denmark has implemented several measures to contain pharmaceutical costs:76
Price regulation: The Danish Medicines Agency (Lægemiddelstyrelsen) regulates the prices of prescription medicines, ensuring they’re sold at the same price across all pharmacies.
Periodic price adjustments: Prices for medicines are reviewed and adjusted every 14 days to encourage competition among manufacturers. In addition, generic substitutions help manage costs, reducing spending on prescription medicines by DKK 3.2 billion (USD 467 million) in 2020. On average, patients save DKK 213 (USD 31) per prescription.77
Reference pricing: Medicines are reimbursed based on the price of the cheapest product within a subsidy group.
The Ministry of the Interior and Health (Indenrigs- og Sundhedsministeriet), the regions, and the The Danish Association of the Pharmaceutical Industry (Lægemiddelindustriforeningen) sets price ceilings for hospital and pharmacy drugs, froze the price cap for subsidy-eligible pharmacy drugs until the end of September 2025, and stipulates that the price of new hospital drugs can’t exceed the average price in nine other European countries.78 In 2023, the cap on annual copayments for reimbursable pharmaceuticals was DKK 3,075 (USD 449).79
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
In 2023, average life expectancy was 81.8 years (about the same as the average for Western Europe) – 79.9 for men and 83.7 for women.80
The top three causes of death in 2022 were:
Neoplasm (cancer): 269 deaths per 100,000 people
Heart disease: 137 deaths per 100,000 people
Diseases of the respiratory system: 108 deaths per 100,000 people.81
The maternal mortality rate was 3.7 deaths per 100,000 live births in 2023 (compared with 11 on average in Europe).82
The avoidable mortality rate was 175 deaths per 100,000 people in 2022.83
The infant mortality rate was three deaths per 1,000 live births in 2023 (compared with seven on average across Europe).84
In 2021, the share of the population with mental health disorders was 16 percent, the same as the average in high-income countries.85
The suicide rate was 11.8 deaths per 100,000 people in 2023, lower than the average of 12 per 100,000 across high-income countries.86
Guns were responsible for 1.1 death per 100,000 in 2023.87
19 percent of adults were affected by severe obesity in 2023.88
In 2023, average life expectancy in Denmark was 81.8 years, slightly higher than the average for high-income countries (79.7 years). Women live about three years longer than men (83.7 years compared with 79.9 years).89
Individuals with only primary-level education experience higher rates of illness, worse health outcomes, and shorter lifespans than people with tertiary education. There are also inequities in survival rates for chronic obstructive pulmonary disease and breast, bowel, and lung cancers.90
Ethnic minorities have higher rates of preterm births and cesarean sections and are less likely to participate in vaccination programs and routine child health checks. Migrant adults also encounter barriers to accessing primary care and dental services and rely more on emergency services.91
Addressing Health Inequities
In 2024, the government announced an agreement to address demographic challenges, reduce health inequities, and enhance local health care access.92 The reform includes:
A new organizational framework to promote collaboration between municipalities and regions
Increased investment in operations, infrastructure, and digital solutions
Redistribution of resources geographically and an increased number of GPs to address inequity
New patient rights related to chronic illness management and the expansion of free health care options near homes
Closer collaboration between physical and mental health services and additional funding for psychiatry.
Several projects have aimed to address health care inequities, including the Danish Health Act (Sundhedsloven) 2019. The PACT project, a national public-private collaboration in the Danish life sciences industry, aims to improve equity by making clinical trials more accessible to provide patients with new treatment options as part of scientific research.93 MOVE, a mobile app that was developed in collaboration with marginalized citizens and health care providers, encourages social connections through exercise.94
Innovation and Reform
Health Care Innovation
The Danish government has implemented a series of reforms to encourage innovation.95 These include:
The Danish Medicines Council (Medicinrådet), which was established to create assessments and guidelines for new medicines in the hospital sector
The Danish Health Technology Council (Behandlingsrådet), which evaluates a wide range of technologies and treatments that could benefit the country’s health care system
Investments to support community hospitals, improve chronic illness care, boost municipal emergency services, advance digital health solutions, and address doctor shortages
Investments in suicide prevention, psychiatric emergency services, and crisis intervention.96
In September 2024, the government released its Health Close to You (Sundhed tæt på dig) reform, which aims to strengthen local health care services and distribute resources and physicians more effectively.97 One proposal is to condense the country’s current five health regions into four, merging the Zealand and Capital regions into a new Eastern Denmark region.
Seventeen new health councils will also be created. The councils will be run collaboratively by regions and municipalities, assume responsibility for local health services, and help centralize decision-making.98
Other initiatives include planning for a “quantum hub” at the University of Copenhagen. Funded by a DKK 40 million (USD 5 million) investment from the Novo Nordisk Foundation, the new hub will develop medicines based on complex calculations of chemical and biochemical processes.99
Health Care Technology
Electronic Health Records
The Danish e-health portal, Sundhed.dk, is the primary platform for accessing public health care services.100 Patients get real-time access to national health registers, medical records, and lab results and are encouraged to take an active role in managing their health care. The portal includes a mobile app, video consultation services, and a digital eHealth card, and it offers access to the shared medication record.101
Telehealth
The COVID-19 pandemic encouraged the adoption of telemedicine technologies and video consultations. In 2022, video consultations became a permanent option. In addition, 83 percent of pharmacies now provide online medicine services.102
The government has allocated DKK 500 million (USD 72 million) from 2023 to 2028 to expand digital treatment services. This investment will focus on:
Reducing physical checkups and preventing unnecessary hospitalizations
Expanding digital psychiatric services, rehabilitation, and municipal screening
Offering digital alternatives to physical visits as appropriate.103
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Morten Schmidt et al., "The Danish health care system and epidemiological research: from health care contacts to database records," Clinical Epidemiology 11 (July 12, 2019):563–91, https://pmc.ncbi.nlm.nih.gov/articles/PMC6634267/.
↩
Activity-based financing is defined as a model where hospitals are funded proportionately to their activity, creating a link between the number and type of patients/conditions treated and the hospitals’ level of income. See Gintare Valentelyte et al., "Analytical methods to assess the impacts of activity-based funding (ABF): a scoping review," Health Economics Review 11, no. 17 (May 18, 2021), https://healtheconomicsreview.biomedcentral.com/articles/10.1186/s13561-021-00315-1.
↩
Statistics Denmark (Danmarks Statistik), Life expectancy, distributed by Statistics Denmark, accessed December 4, 2025, https://www.dst.dk/en/Statistik/emner/borgere/befolkning/middellevetid; Austin E Schumacher et al., “Global age-sex-specific all-cause mortality and life expectancy estimates for 204 countries and territories and 660 subnational locations, 1950–2023: a demographic analysis for the Global Burden of Disease Study 2023.” The Lancet 406, no. 10513 (October 18, 2025):1731–1810, https://doi.org/10.1016/S0140-6736(25)01330-3.
↩
Institute for Health Metrics and Evaluation, GBD compare, distributed by IHME, accessed December 4, 2025, https://vizhub.healthdata.org/gbd-compare/; overall firearm mortality is the aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.