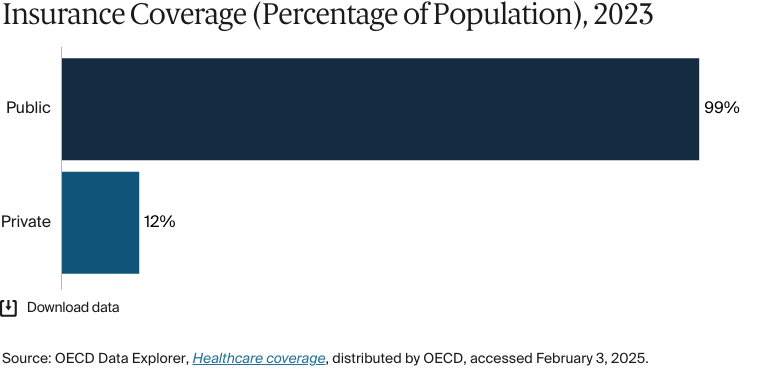
Türkiye’s universal health insurance system (Genel Sağlık Sigortası) reaches 99 percent of the population. The system covers many essential services, although some copayments are required. About 12 percent of people supplement government health care with private insurance.
While the Social Security Institution, a government agency, is responsible for ensuring universal health coverage, the health system operates through a hybrid public-private structure. Public health care is funded mainly by employers, employees, and the state.
Türkiye’s health system has improved significantly since its Health Transformation Program introduced universal insurance and expanded access. However, persistent challenges remain, including a shortage of health care professionals and urban–rural disparities. In addition, the country has hosted the highest number of refugees globally for the last 11 years, including nearly three million Syrian migrants, who face significant barriers to accessing medical care. Health care spending as a share of gross domestic product is the lowest among the 38 member states of the Organisation for Economic Co-operation and Development.
Between 2003 and 2013, Türkiye implemented its Healthcare Transformation Program (HTP), creating a comprehensive roadmap toward universal health care. Once the new program had taken effect, the proportion of the population with coverage grew dramatically: from less than two-thirds to more than 99 percent by 2022.
Public insurance coverage: 99% of population
Private insurance coverage: 12.10% of population
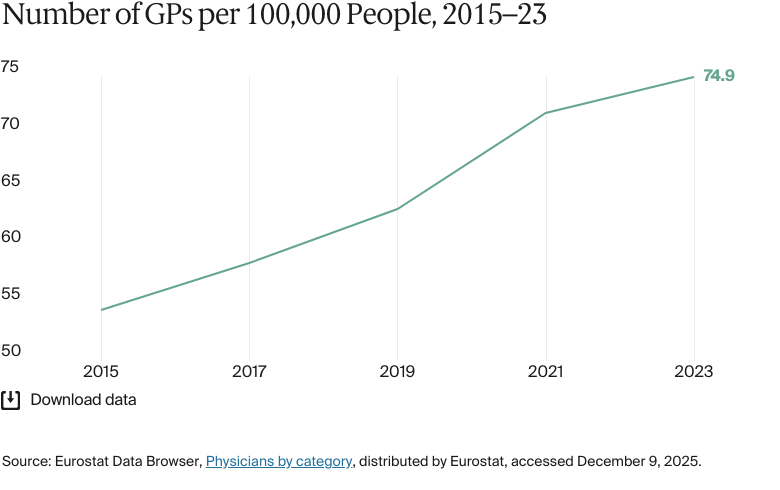
Primary care physicians: 74.9 per 100,000 people
Specialist physicians: 133 per 100,000 people
Total health care spending in Türkiye was USD 40.6 billion in 2022. In 2022, the country’s per capita spending on health care was the equivalent of USD 482.
Pharmaceutical spending: N/A
Out-of-pocket spending: 19.05% of total health care spend
Health care access in Türkiye is divided along socioeconomic lines.
While most citizens rely on government-funded hospitals, wealthier people can access world-class private facilities. There are regional disparities in the density of doctors that have persisted despite the introduction of measures such as bonus payments and higher salaries to attract health workers to underserved areas. Doctors are also required to spend some time in more deprived areas of the country after the end of their training.
Türkiye’s Ministry of Health (Türkiye Cumhuriyeti Sağlık Bakanlığı) was established in 1920, and the groundwork for today’s public health system was laid between 1923 and 1946.1 Between 1946 and 2002, the country set up various public health insurance funds for different groups, including workers, retirees, and the self-employed.2
Throughout the 20th century, Türkiye embarked on numerous health care reforms, such as the 1946 First 10-Year National Health Plan which aimed to expand services and improve infrastructure; the 1961 Socialization of Health Services Law which focused on integrated primary care and rural outreach; and the 1993 National Health Policy which focused on environmental health and health care delivery. However, none of these were ever fully realized because of political instability, legal and bureaucratic barriers, and economic constraints.3
As a result of the incomplete reforms, the country’s health system struggled to meet the population’s needs. In 2002, less than two-thirds of the population had public health insurance, and access to health services was highly fragmented and varied significantly by region.4
Between 2003 and 2013, Türkiye implemented its Healthcare Transformation Program (HTP), creating a comprehensive roadmap toward universal health care.5 An important part of the transformation occurred in 2006, when five existing insurance programs were merged into one, forming the General Health Insurance Scheme (Genel Sağlik Sigortası, or GSS). This made social health insurance compulsory for all and created the Social Security Institution (Sosyal Güvenlik Kurumu, or SGK), which manages and funds the program.6 Once the new program had taken effect, the proportion of the population with coverage grew dramatically: from less than two-thirds to more than 99 percent by 2022.7
The Role of Public Health Insurance
Today, the GSS provides comprehensive coverage to most long-term residents. Certain groups are covered unconditionally; this coverage includes health services for children, long-term medical care, infectious disease treatment, substance abuse prevention services, maternity care, and emergency care. The government also guarantees coverage for recipients of social benefits and for those with a per capita household income below one-third of the gross minimum wage. Foreign nationals are eligible if they hold a residency permit, have lived in Türkiye for at least one year, and do not have health insurance from another country.8
The system is financed through a mix of employer and employee contributions, government funding, and out-of-pocket payments. Employers must enroll their employees automatically and contribute 12.5 percent of the employees’ earnings (with 7.5% paid by the employer and 5% by the employee). Self-employed individuals obtain coverage by paying 12.5 percent of their declared income. Unemployed individuals who are not covered by social benefits must pay 3 percent of the national gross minimum wage unless they qualify for government support through a means test.9
Inpatient care (private hospitals may charge additional fees)
Outpatient care (some services are subject to copayments)
Maternity care
Primary care
Pharmaceuticals (for prescribed medications)
Dental care (orthodontic treatment is covered for individuals under age 18)
Eye care (including glasses up to a fixed price limit)
Mental health care
Rehabilitative care
Home visits
Assistive devices (with coverage up to fixed price limits).
Outpatient care is covered for services provided by public primary care providers such as family physicians, but copayments are required for outpatient care received at public, university, and private hospitals.11
Maternity care covers pregnancy checkups, delivery, and postnatal care. Up to three rounds of in vitro fertilization treatment are partially covered for married couples; the copayment is 30 percent for the first round and 20 percent for the third.12
To get coverage for glasses, patients must receive a prescription from an ophthalmologist. Copayments apply if the price exceeds the set limit. Patients can typically replace their glasses every three years, and contact lenses can also be covered in certain cases.13
Assistive devices provided in inpatient settings are covered mostly under the case-based payment method, under which hospitals receive a fixed payment for treatment. However, some specialized devices may require separate invoicing and are sometimes not fully covered. In outpatient care, patients must purchase the device and submit a receipt for reimbursement, up to a set limit. If the cost exceeds this limit, copayments apply: pensioners pay 10 percent, while others pay 20 percent.14
Long-term care (institutional care is limited, and most care is provided by family members at home).16
Safety Nets
Türkiye’s public health care system includes several safety nets:
Prescription medications: The SGK subsidizes or provides free prescription medications for low-income individuals, children, and people with chronic conditions.17
Support for people with low incomes: The government provides full coverage for those whose per capita household income is below one-third of the gross national minimum wage (seeThe Role of Public Health Insurance).18
Maternal and children’s health care: Women receive free or subsidized prenatal and postnatal care. Children’s health care is also covered, including vaccinations.19
Chronic illness and disability support: Free or subsidized health care services, including medications, are available for individuals with disabilities.20
The Role of Private Health Insurance
About 12.1 percent of the Turkish population had private health insurance in 2022, a rise from 2.8 percent in 2010.21
The SGK has agreements with many private hospitals to offer discounted care for residents, but patients are usually responsible for some out-of-pocket expenses. To help pay for these unexpected costs, many residents purchase complementary health insurance plans, which cover some of the expenses that are not fully paid by the SGK.22
The Role of Government
Following the HTP reforms between 2003 and 2013, the management of the Turkish health system became highly centralized.23 In 2019, as part of the country’s transition from a parliamentary system to a presidential republic, the health system was further centralized under the Health and Food Policies Council and, ultimately, the president of Türkiye. The Ministry of Health and its regional offices implement centrally decided policies.24
In 2010, the government launched a public-private partnership (PPP) program to improve health care access and quality. In this model, the private sector finances, constructs, and maintains health care facilities, while the Ministry of Health is responsible for providing medical services. This approach has increased bed capacity and improved service quality and efficiency in health care delivery.25
Integration and Care Coordination
Türkiye has made progress in care coordination through the implementation of its digital health infrastructure and efforts to strengthen primary care. For instance, the digital health platform e-Nabız (“e-Pulse”), introduced in 2015 and since made available nationwide, allows patients to access their medical records and health care providers to share data (seeHealth Care Innovation).26
In 2011, the country introduced a family practitioner initiative, making family physicians and family health centers the main providers of preventive and curative services. Community health centers support public health, logistics, and services not covered by family physicians.27
But gaps remain in the integration of different levels of care. For example, family medicine centers and healthy living centers operate on separate databases, even though the former supports the latter. The lack of integration between these complementary facilities, which offer a range of preventive care and chronic disease management services, makes the seamless coordination of patient care difficult to achieve. Additionally, with no formal referral pathways or standardized work protocols linking primary care with secondary care, patients can experience problems navigating their health care.28
While government leaders at both the national and local levels have said that they are strongly committed to improving care coordination, frequent structural changes within the Ministry of Health and fragmented policies have slowed the implementation of coordinated approaches and made it difficult to create a consistent strategy across the health care system.29
Operations and Resources
Overview of the Delivery System
Türkiye’s public health care system is made up of a comprehensive network of providers that can be broadly categorized into three groups:
Primary care is mainly provided through family health centers (aile sağlığı merkezleri, or ASM), which offer essential health services, such as preventive care, maternal and children’s health services, and the management of chronic diseases.30
Secondary care is more specialized medical care that is provided by public and private hospitals, which are typically the first point of referral from primary care.31
Tertiary care includes advanced specialist services, transplants, and high-complexity treatments that are delivered in university hospitals.32
Community health care is also an important part of the delivery system. It’s delivered through community health centers (toplum sağlığı merkezleri, or TSM; seePrimary Care), with home visits for eligible patients and mobile health units operating in rural areas.33
Primary Care
The strength of Türkiye’s primary health care system is largely due to the introduction of the family medicine program as part of the HTP. This program now forms the backbone of the country’s primary health care services.34
A pilot project launched in 2005 required all state-funded primary care to be delivered through ASM; this policy was expanded nationwide by 2010 and reinforced in 2011. People normally visit their assigned family doctors at their designated ASM.
Healthy living centers (sağlıklı hayat merkezleri, or SHM) complement family medicine centers by providing preventive services, chronic disease management, and lifestyle interventions.35 TSM support family practitioners by promoting public health and offering logistical support. As of 2020, the country had 8,015 ASM, 779 TSM, and 216 SHM.36
ASM are typically staffed by a family medicine physician, a nurse, and one or two medical assistants.37 As of 2019, each family medicine physician is responsible for an average of 3,378 patients.38
Family medicine in Türkiye operates under a capitation system, where physicians are paid a set amount for every patient. In regions with a higher proportion of low-income residents or rural populations, the payment rate is adjusted upward to account for additional challenges, such as workforce shortages. Family medicine practices can also earn additional payments or face penalties based on the quality of care provided, with quality measures considering areas such as prenatal care coverage, immunization rates, and the adequacy of facilities.39
There were 74.9 practicing general practitioners (GPs) for every 100,000 people in 2023.40 There are no data available for the proportion of primary care physicians employed publicly versus privately.
Outpatient/Specialist Care
Specialized care is provided by hospital outpatient departments, private doctors, and private outpatient centers.41
Initially, the family medicine reform program component of the HTP required that patients be referred for specialized care by their family doctors; patients who chose to skip this referral process were subject to copayments. However, because this policy put the burden to reduce overcrowding in secondary (specialist) care on family doctors, the policy was later reversed by the Ministry of Health.42
With no gatekeeping of secondary care, Turkish patients tend to overuse services such as hospitalization and diagnostic tests.43 Copayments for outpatient services covered by public insurance in hospitals and health centers encourage the use of family doctors, driving a shift from inpatient to outpatient care.44
Türkiye had only 133 specialist medical practitioners for every 100,000 people in 2022.45 There are no data available for the proportion of specialist medical practitioners employed publicly versus privately.
Physician Education and the Workforce
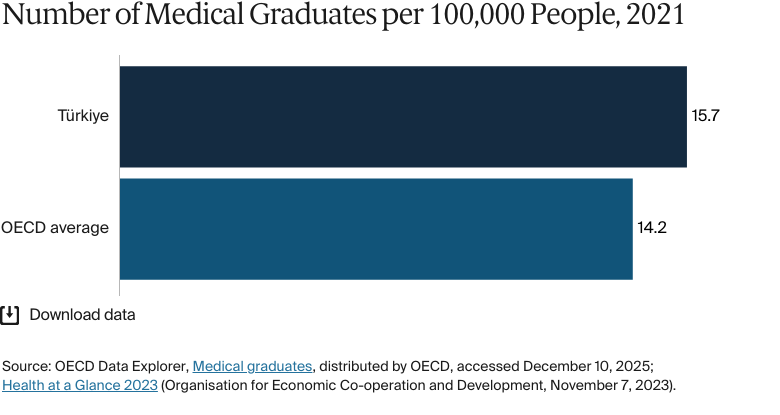
In 2021, there were 15.7 medical graduates for every 100,000 people in Türkiye, compared with 14.2 across Organisation for Economic Co-operation and Development (OECD) countries.46 There were 68 university hospitals in 2022.47
The country is a popular destination for foreign students, who are attracted by low fees and government initiatives such as the Türkiye Scholarships. Many universities offer courses taught in English as well as Turkish.48 Fees vary between public and private institutions and depending on whether programs are taught in English or Turkish. The cost of private medical school ranges from USD 14,000 to USD 27,500 per year.49
There are no data available for the proportion of the workforce recruited from overseas or who choose to work overseas.
One of the main aims of the HTP was to expand the supply of health workers. Initiatives run between 2003 and 2010 increased the number of university places, offered improved salaries with performance-based remuneration, and created more flexible contracts. New doctors are also required to work in underserved regions once their training has concluded. They receive bonus payments and higher salaries if they choose to work in these areas at a later point in their careers.50
Many health systems are under stress, and the demand for more care is not being met by sufficient health workers — especially in rural or underserved areas. The public is asking for better, faster care [at the same time] as the health workforce is asking for fewer hours, fewer shifts, higher pay.
Dr. Margaret Kruk
Harvard T.H. Chan School of Public Health
Hospitals
BY THE NUMBERS
In 2022, there were 348 nurses per 100,000 people (compared with an average of 826 across Europe).51
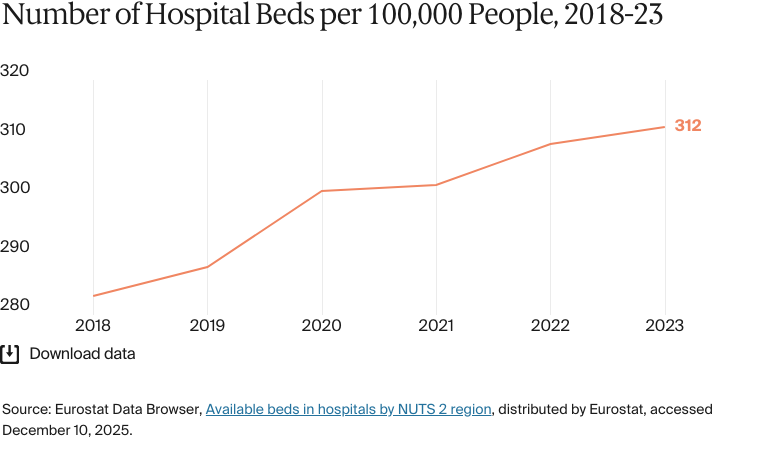
In 2023, there were 312 hospital beds per 100,000 people (compared with 374 across upper-middle-income countries in 2022.52
There are three main types of hospitals in Türkiye: public hospitals owned by the Ministry of Health, university hospitals specializing in tertiary care, and privately owned secondary care hospitals.53
In 2022, the country had 1,555 hospitals: 915 public hospitals, 68 university hospitals, and 572 private hospitals.54 There were 312 hospital beds for every 100,000 people in 2023, below the average of 374 for every 100,000 people across upper-middle-income countries in 2022.55
The Turkish government has used a PPP model to increase bed numbers as part of its Health PPP Program first launched in 2010.56 Led by the Ministry of Health, the initiative consists of about 30 integrated health campuses known as city hospitals which will have a collective capacity of 43,000 beds.57
Mental Health Care
BY THE NUMBERS
In 2023, there were eight psychiatrists per 100,000 people (compared with 10 in Europe in 2024).58
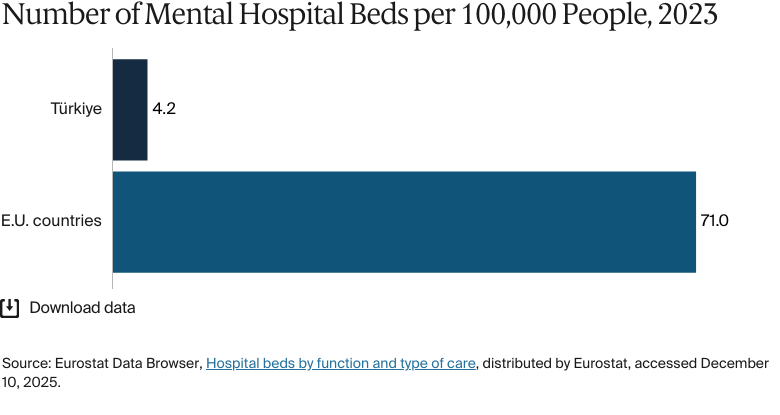
In 2023, there were 4.2 mental hospital beds per 100,000 people (compared with 71 in European Union [E.U.] countries).59
Out of a population of about 85.3 million, about 9million people seek mental health support in Türkiye each year.60 There is a need for more provision, with only 4.2 mental hospital beds for every 100,000 people in 2023, compared to 71 across E.U. countries.61
The country has started to shift toward a community model of mental health treatment. Between 2011 and 2016, 175 community mental health centers were established to support individuals with mental health issues, although 50 percent of psychiatric inpatient beds were still in psychiatric institutions as of 2021.62
Türkiye’s large refugee population faces barriers to accessing mental health care.63 In a sample study, 14.8 percent of refugees had expressed the need for mental health care since arriving in the country, but language barriers and a lack of information meant only 1.4 percent were able to access support.64 The Turkish government works closely with the World Health Organization to run the Refugee Health Program, which aims to improve refugees’ access to health care and offers mental health training to Turkish and Syrian health care providers.65
Long-Term Care and Social Support
Projections indicate that the proportion of the population age 65 and over in Türkiye will increase from 9.1 percent in 2019 to 12.9 percent by 2030 and 22.6 percent by 2060.66
Formal long-term care services, such as nursing homes and elderly care centers, are limited, and the system relies heavily on informal, family-based support.67 Traditionally, families care for elderly and disabled individuals at home. The Ministry of Family and Social Services (Aile ve Sosyal Hizmetler Bakanlığı) is responsible for providing services to the elderly and disabled.68 To assist low-income families, the ministry provides financial support by paying family members who care for low-income people with disabilities at home.
As of August 2024, low-income families receive TRY 9,077 (USD 264) monthly to support the home care of fully dependent individuals with disabilities.69 Eligibility is means-tested: the household’s per capita income must be less than two-thirds of the net minimum wage. Higher-income families are ineligible for subsidies.70
The Ministry of Family and Social Services also oversees the country’s formal long-term care facilities, which tend to be concentrated in urban areas. The private sector has expanded its role in long-term care, with private nursing homes and care facilities emerging to meet growing demand. However, these services are costly and inaccessible for many citizens.71
Cost and Affordability
Health Care Spending Overview
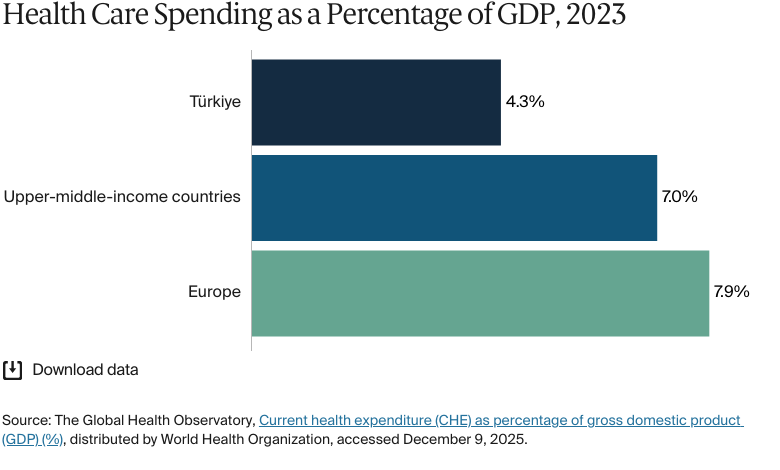
Total health care spending in Türkiye was USD 40.6 billion in 2022.72 In 2022, the country’s per capita spending on health care was the equivalent of USD 482, compared with USD 585 across upper-middle-income countries.73 In 2023, the country spent 4.3 percent of its gross domestic product (GDP) on health care, compared with 7.9 percent across Europe.74
In 2024, government funding accounted for 76.1 percent ofhealth expenditure, out-of-pocket spending accounted for 18.8 percent, and private insurance accounted for 2.8 percent.75
Pharmaceutical Spending
In 2022, Türkiye’s per capita spending on pharmaceuticals was USD 91, compared with USD 490 across OECD countries.76
Pharmaceutical spending has been increasing as a result of the country’s growing health care needs and the development of its pharmaceutical industry, which ranks 11th among European nations by market size.77
Based on pricing data published in annual pharmaceutical market reports between 2015 and 2023, brand-name medications were much more costly than generic medications. By 2023, the average price of brand-name medicines had reached over TRY 134 (USD 4) per item, compared with generic medicines, which were TRY 47 (USD 1) per item.78
Türkiye has implemented several measures to manage pharmaceutical costs. A reference pricing system, for instance, sets maximum retail prices for drugs by comparing their prices with the lowest prices in five designated European countries. The government also promotes the use of cheaper generic alternatives to reduce overall spending while maintaining access to essential medicines.79
There’s also a fixed exchange rate for pricing imported pharmaceuticals, which can mitigate the cost impact of rate fluctuations. Reimbursement policies determined by the SGK also support access to essential medications by defining which drugs qualify for reimbursement.80
Cost Sharing and Out-of-Pocket Spending
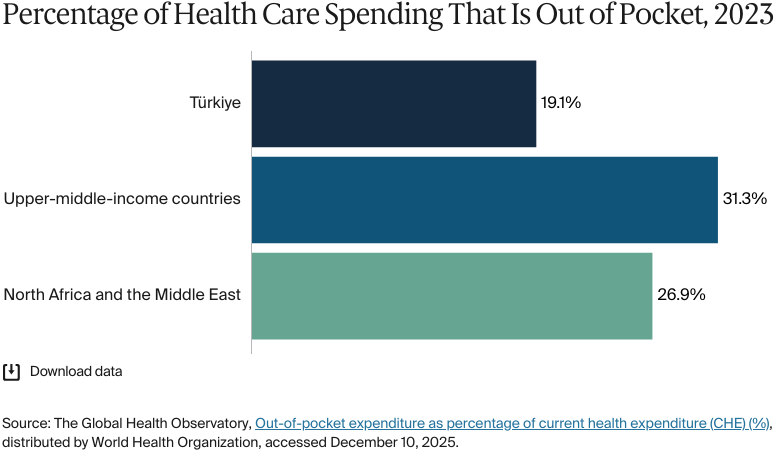
In 2024, household out-of-pocket spending made up 19.05 percent of total health care spending, compared with an average of 31.3 percent across upper-middle-income countries in 2023.81 Out-of-pocket expenditure per capita was USD 92 annually in 2022, compared with USD 182 across upper-middle-income countries.82
The GSS partially covers prescription drugs and requires copayments. Generally, patients pay about 20 percent of the costs of medications out ofpocket, with retirees paying 10 percent.83 Primary care facilities do not require a copayment. Copayments are required for outpatient visits at a fixed rate.84
Many people are struggling to meet rising health care costs. Medical inflation is high: The health sector’s inflation rate was 53.5 percent in August 2024. While this is a decrease from the previous month’s63 percent, it still exceeds the long-term average of 28 percent.85
Rates of unmet medical needs as a result of distance, cost, or wait times have decreased markedly since 2010. In 2020, only 1.9 percent of the population reported foregoing a medical examination for these reasons — a similar proportion to the E.U. average.86
Fewer Turkish households face catastrophic health expenditure than is the case in some European countries. However, half of those that do are already unable to meet their basic needs.87
How Are Costs Contained?
Türkiye is using several strategies to try to contain health care costs while maintaining quality and accessibility. These include:
PPPs to develop and operate health care facilities, with the goal of improving infrastructure and service quality while controlling public spending.88
Pharmaceutical pricing controls to regulate drug prices using external reference pricing and fixed exchange rates.89
Health technology assessments to evaluate the cost-effectiveness of new medical technologies and treatments and to direct health care spending toward high-value interventions.90
Quality and Outcomes
BY THE NUMBERS
Life expectancy at birth was 78.1 years in 2022–2024 (compared with 73.7 years for North Africa and the Middle East in 2023):
Life expectancy for women was 80.7 years in 2022–2024 (compared with 73.7 years for North Africa and the Middle East in 2023).
Life expectancy for men was 75.5 years in 2022–2024 (compared with 73.7 years for North Africa and the Middle East in 2023).91
The avoidable mortality rate was 287 per 100,000 people in 2023.92
The top three causes of death in 2024 were:
Diseases of the circulatory system: 206 deaths per 100,000 people
Neoplasms: 93 deaths per 100,000 people
Diseases of the respiratory system: 86 deaths per 100,000 people.93
The maternal mortality rate was 11 deaths per 100,000 live births in 2023, in line with the average across Europe.94
The infant mortality rate was nine deaths per 1,000 live births in 2023 (compared with 11 on average across Europe and Central Asia in 2023).95
In 2021, the share of the population with mental health disorders was 16 percent.96
The suicide rate was 4 deaths per 100,000 people in 2023, compared with seven across upper-middle-income countries.97
In 2023, guns were responsible for three deaths per 100,000 people.98
33 percent of adults were affected by obesity in 2022, compared with an average of 16 percent across upper-middle-income countries.99
Health Outcomes
Türkiye’s median age is 34 years, significantly younger than the E.U. average of 44.5 years.100 The country also has a high obesity rate: In 2022, 33.3 percent of its adult population was classified as obese, compared with 15.8 percent across upper-middle-income countries.101
The introduction of the HTP improved access to obstetric care and introduced free health care coverage for children, leading to a large decrease in infant mortality.102 The rate of infant mortality was nine deaths for every 1,000 live births in 2023, compared with 30.7 in 2000.103
In 2023, the overall avoidable mortality rate was 287 deaths for every 100,000 people, with significant differences between genders: 368 deaths for every 100,000 men, compared with 211 deaths for every 100,000 women.104
Addressing Health Inequities
Health care access in Türkiye is divided along socioeconomic lines. While most citizens rely on government-funded hospitals, wealthier people can access world-class private facilities.
There are regional disparities in the density of doctors that have persisted despite the introduction of measures such as bonus payments and higher salaries to attract health workers to underserved areas. Doctors are also required to spend some time in more deprived areas of the country after the end of their training.105
For the past 11 years, Türkiye has hosted the highest number of refugees globally. For example, by the end of 2024, the country was hosting more than 2.5 million Syrian nationals under temporary protection (TP), as well as nearly 200,000 applicants for international protection (IP).106 Entitlement to health care and systems for access vary between IP and TP. IP applicants can access free care under the GSS for one year, after which they must pay health insurance premiums.107
Systems also vary by region. Once the one-year entitlement ends, IP applicants in Istanbul are categorized as health tourists and must pay much higher prices; in Izmir, IP applicants must prove they have a medical need to access care.108 IP applicants also face issues accessing care outside the city where they registered.109
TP applicants are covered by the GSS (with no one-year limit) but must pay a contribution fee.110 The premiums TP applicants pay are determined by an income test, with the lowest earning group having their premiums covered.111 Through the SIHHAT Project (“Supporting Integrated Health Healthcare Access for Temporary Protection”), Türkiye (with help from E.U. funding) has established 190 migrant health centers which are focused on treating Syrian refugees. Because TP beneficiaries are only entitled to care in their province of registration, except in circumstances where treatment is not available, there can be significant barriers to receiving care.112
Türkiye has made substantial progress in reducing regional health disparities over the past decade, mainly through the HTP, launched in 2003. This program expanded the GSS, culminating in nearly total coverage.113 The HTP also eased financial barriers for low-income individuals by reducing out-of-pocket health care costs.114
The family medicine reform component of the HTP included a requirement to shift doctors from urban centers with high doctor-to-population ratios to rural areas with shortages. This has helped to reduce inequities in care.115
The Elderly Support Program (Yaşlı Destek Programı, or YADES), introduced in 2016, funds municipal home care and social services for older adults.116 YADES aims to reduce disparities by ensuring that elderly individuals, especially in underserved areas, receive essential care at home rather than in institutional services concentrated in urban centers. Since its inception, the program has funded 74 projects across 42 municipalities, reaching 128,691 elderly individuals in 87,987 households.117
Innovation and Reform
Health Care Innovation
Türkiye is implementing reforms to improve health care access, quality, and efficiency. The Ministry of Health’s 2024–28 Strategic Plan includes 40 goals across five areas: promoting healthy living, strengthening primary care, enhancing service quality, developing institutional capacity, and advancing national health care technology.118
Value-based health care, meanwhile,is transforming the system by prioritizing patient outcomes ahead of service volume. Supported by partnerships with global organizations, it uses data-driven strategies, continuous professional training, and cost-efficiency measures to improve care.119
Health Care Technology
The e-Nabız system, which had been adopted by 80 percent of the population by 2022, integrates electronic health records across more than 28,000 health facilities. The platform enables seamless access to medical records, which should reduce errors and enhance care coordination.120
The Ministry of Health has also partnered with the Healthcare Information and Management Systems Society (HIMSS), a global nonprofit organization, to improve digital maturity within the health system using training and workshops in areas such as analytics and digital imaging.121
Telemedicine has expanded through the 2022 Regulation on Remote Health Services, enabling consultations, e-prescriptions, and even surgical procedures.122 These services bridge gaps in rural health care access and reflect Türkiye’s focus on using technology to make care more equitable.
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Universal Health Insurance System in Turkey (Türkiye’de Genel Sağlık Sigortası Sistemi için tıklayınız) (Social Security Institution [Sosyal Güvenlik Kurumu]), accessed January 30, 2025, https://www.sgk.gov.tr/YayinveProjeler/Yayinlar/7f65e722-ba64-48df-a5ca-c60336c2fbc5; an overview of Turkey’s Universal Health Insurance system, detailing its history, structure, financing, coverage, and IT infrastructure.
↩
9
Social Security Institution, Universal Health Insurance.↩
10
Social Security Institution, Universal Health Insurance.↩
11
Social Security Institution, Universal Health Insurance.↩
12
Social Security Institution, Universal Health Insurance.↩
13
Social Security Institution, Universal Health Insurance.↩
14
Social Security Institution, Universal Health Insurance.↩
15
Fahad Ahmed et al., “Palliative care in Turkey: insights from experts through key informant interviews.” Journal of Cancer Policy 42 (December 2024):100506, https://doi.org/10.1016/j.jcpo.2024.100506.
↩
Safir Sumer et al., Building an Improved Primary Health Care System in Turkey Through Care Integration (World Bank Group, July 17, 2019), https://doi.org/10.1596/33098.
↩
Zeynep Güldem Ökem and Mehmet Çakar, “What have health care reforms achieved in Turkey? An appraisal of the ‘Health Transformation Programme’.” Health Policy 119, no. 9 (September 2015):1153–63, https://doi.org/10.1016/j.healthpol.2015.06.003.
↩
Engin Karadag, “International medical students in Türkiye: a cross-sectional study on their reasons for choosing Türkiye and their demographic and socioeconomic characteristics.” BMC Medical Education 24 (October 19, 2024):1171, https://doi.org/10.1186/s12909-024-06200-9.
↩
H Semih Yildirim, “The financial architecture of Turkish healthcare PPPs.” International Journal of Business and Management Studies 4, no. 6 (June 2023):14–20, https://ijbms.net/assets/files/1689098675.pdf.
↩
Eurostat Data Browser, Hospital beds by function and type of care, distributed by Eurostat, accessed December 10, 2025, https://doi.org/10.2908/HLTH_RS_BDS1.
↩
Cengiz Kiliç, “Barriers to accessing mental health services among Syrian refugees: a mixed-method study.” Turkish Journal of Psychiatry 35, no. 2 (2024):87–94, https://doi.org/10.5080/u27044.
↩
65
World Health Organization, “Supporting Turkish mental health.”
↩
“Our mission and vision” (Misyon ve vizyonumuz), Turkish Ministry of Family and Social Services (Aile ve Sosyal Hizmetler Bakanlığı), accessed May 14 2025, https://www.aile.tr/eyhgm/genel-mudurluk/misyon-ve-vizyonumuz; an overview of the mission and vision of the Directorate General for Services for Persons with Disabilities and the Elderly.
↩
Enver Kagan Atikeler and Gulbin Özçelikay, “Comparison of pharmaceutical pricing and reimbursement systems in Turkey and certain EU countries.” SpringerPlus 5 (October 26, 2016):1876, http://doi.org/10.1186/s40064-016-3455-z.
↩
Atikeler and Özçelikay, “Comparison of pharmaceutical pricing.”
↩
90
E. Kağan Atikeler et al., “Health technology assessment in Turkey: current status and perspectives on future implementation.” Health Policy and Technology 12, no. 1 (March 2023):100701, https://doi.org/10.1016/j.hlpt.2022.100701.
↩
91
Data Portal for Statistics, Life tables, 2022–2024, distributed by Turkish Statistical Institute, accessed December 10, 2025, https://data.tuik.gov.tr/Bulten/Index?p=Life-Tables-2022-2024-54081; Austin E Schumacher et al., “Global age-sex-specific all-cause mortality and life expectancy estimates for 204 countries and territories and 660 subnational locations, 1950–2023: a demographic analysis for the Global Burden of Disease Study 2023.” The Lancet 406 (October 18, 2025):1731–1810, https://doi.org/10.1016/S0140-6736(25)01330-3.
↩
“Suicide Rates by Country,” World Population Review, accessed January 21, 2026, https://worldpopulationreview.com/country-rankings/suicide-rate-by-country.
↩
98
Institute for Health Metrics and Evaluation, GBD compare, distributed by IHME, accessed April 20, 2025, https://vizhub.healthdata.org/gbd-compare; overall firearm mortality is the aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.