Spain’s national health system (Sistema Nacional de Salud) provides universal health coverage to all residents, including asylum seekers and undocumented migrants. The system is decentralized, with 17 autonomous communities managing health care planning, financing, and service delivery and is primarily funded through general taxation, with additional contributions from copayments, out-of-pocket payments, and public-private partnerships. Health services are free at the point of use, except for certain pharmaceuticals, dental services, and orthoprosthetic devices, all of which require income-based copayments.
Life expectancy in Spain is high, and the country sees one of the lowest avoidable mortality rates in the European Union, but the system faces significant challenges, including long wait times, workforce shortages, and hospital capacity constraints. Efforts are under way to modernize infrastructure and improve integration between care services to address these issues.
The Spanish National Health System (Sistema Nacional de Salud — the SNS) provides coverage to legal residents, including asylum seekers and refugees, as well as to documented and undocumented migrants. The system is primarily financed through taxation, with additional contributions from copayments, out-of-pocket payments, mutual funds, the European Union (E.U.), and public-private partnerships. All eligible individuals are automatically covered by the SNS’s common package of benefits.
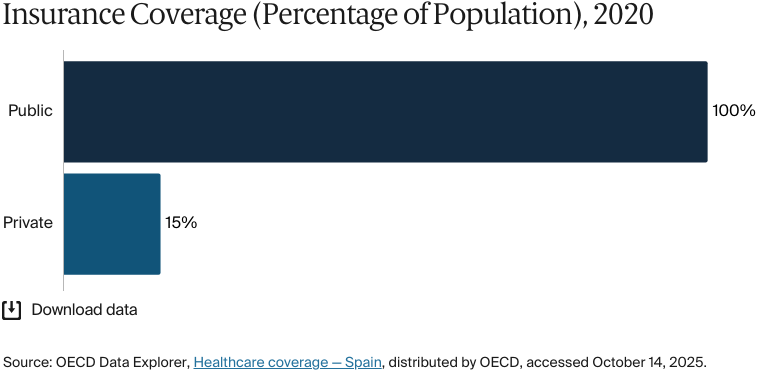
Public insurance coverage: 100% of population
Private insurance coverage: 26.4% of population
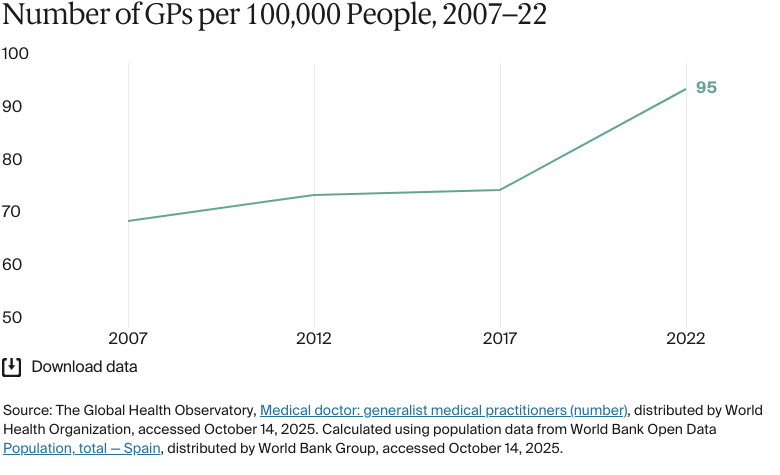
Primary care physicians: 95 per 100,000 people
Specialist physicians: 283 per 100,000 people
Health care spending has steadily increased. In 2022, per capita health expenditure was USD 3,320. The largest contributor to health expenditure is public funding: 74 percent of spending in 2022, up from 70.3 percent in 2018.
Pharmaceutical spending: 15% of total health care budget
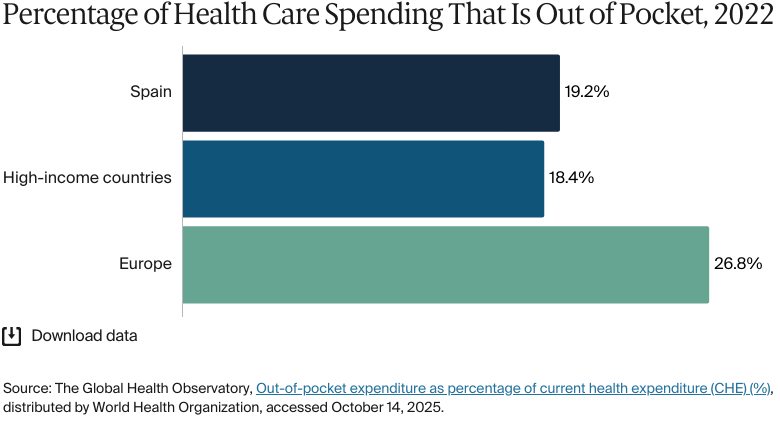
Out of pocket spending: 20.9% of total health care spend
In 2024, 25.8 percent of the population was at risk of poverty or social exclusion. In 2019, 49.2 percent of women ages 20 to 69 in the lowest income quintile underwent cervical cancer screening, compared with 65.3 percent in the highest quintile. Disparities in self-rated health exist between immigrants and native Spaniards, particularly among those residing in Spain for six to 15 years.
Despite SNS coverage, homeless individuals and asylum seekers face significant barriers to accessing health care. The Roma community, which accounted for 2 percent of the population in 2020, faces lower life expectancy, higher rates of chronic diseases, poor nutrition, and low vaccination rates, largely due to persistent socioeconomic disadvantage, barriers to health care access, and systematic discrimination. The LGBTQ+ community also experiences higher rates of mental health issues, as well as less access to services for preventing HIV/AIDS and testing for sexually transmitted infections.
Spain introduced mandatory health insurance in 1942 — a social security system funded through payroll contributions. Between 1942 and 1977, the system was centrally managed by government institutions. This model remained in place for several decades.1
In 1978, the Spanish Constitution laid the groundwork for decentralization. Over the years that followed, responsibilities for health care planning and public health management gradually transferred to Spain’s 17 autonomous communities. This process concluded in 2002, at which time the regional governments assumed full control of health service delivery.2
A significant structural reform came in 1986, with the Health Care General Act. This law began the transformation from a social security system to a national health service, shifting financing from payroll contributions to general taxation. The transition was completed in 1999, with the formation of the Spanish National Health System (Sistema Nacional de Salud — the SNS), which today provides universal coverage.3
The Council of the National Health System now ensures coordination between the government, autonomous communities, and autonomous cities of Ceuta and Melilla.4
The Role of Public Health Insurance
The SNS provides coverage to legal residents, including asylum seekers and refugees, as well as to documented and undocumented migrants.5
The system is primarily financed through taxation, with additional contributions from copayments, out-of-pocket payments, mutual funds, the European Union (E.U.), and public-private partnerships (see Health Care Spending Overview).6
All eligible individuals are automatically covered by the SNS’s common package of benefits, which is divided into three subcategories. The differences between these concern the nature of the services offered and the way they are financed, particularly regarding copayments:7
The basic package covers primary care, specialized care, hospital stays, emergency services, and preventive care. It’s free at the point of use.
The supplementary package includes pharmaceuticals and certain orthoprosthetic devices, such as wheelchairs. Copayments are based on income.
The accessory package was created in 2012 to designate nonessential services that could be subject to cost sharing. However, this package was never clearly defined or implemented, and no related regulation had been issued as of 2024. A new draft law under parliamentary review proposes eliminating this category entirely.
The autonomous communities can expand this to cover additional services, but they must demonstrate financial viability and notify the Council of the National Health System in advance.8
Services Covered by Public Health Insurance
Services that are covered by the common package are as follows:9
Preventive care
Inpatient care
Outpatient care
Maternity care
Primary care
Pharmaceuticals (some copayments required)
Dental care (but only for basic preventive services)
Mental health care
Palliative care
Long-term care
Rehabilitation
Home visits
Assistive devices.
Inpatient medicines are fully covered; outpatient prescriptions require copayments. For most chronic conditions, patients pay 10 percent of the retail price, with a cap of EUR 4.24 (USD 4.6) per prescription (see Pharmaceutical Spending).10
Some autonomous communities have expanded dental coverage beyond basic preventive services within their common package of benefits. However, coverage is often limited to certain age groups or clinical conditions, and specific services offered vary by region.11
The SNS doesn’t cover optical care or specialized dental treatments, such as orthodontics.12
Safety Nets
Spain has one of the lowest rates of catastrophic health care spending in the E.U.13 In 2020, 2.9 percent of households faced catastrophic health expenses.14
Some groups qualify for full or partial exemptions from copayments: low-income individuals (including pensioners) eligible for welfare benefits, unemployed people who are no longer eligible for unemployment benefits, patients with work-related ailments, disabled adults and children, and households receiving the child benefit.15
For pensioners who are not covered by one of the mutual funds (see The Role of Private Health Insurance), monthly spending caps on outpatient prescriptions range from EUR 8.23 (USD 8.6) for annual incomes under EUR 18,000 (USD 18,729) to EUR 61.8 (USD 64.3) for annual incomes over EUR 100,000 (USD 104,052).16
Orthoprosthetic devices have item-specific caps that are independent of income level, ranging from EUR 0 to EUR 36 (USD 39).17
The Role of Private Health Insurance
In 2020, 15.3 percent of the population had private health insurance.18 In 2024, this number had risen to 26.4 percent.19
In February 2025, the government reported that private health care spending accounted for 2.6 percent of Spain’s gross domestic product (GDP).20 Additionally, in 2024, 10.1 percent of public health care expenditure was allocated to public-private collaborations.21
Private health insurance is most popular in the capital, Madrid, and in the autonomous communities of Catalonia and Andalusia, where 57 percent of Spain’s private hospitals are located.22 People ages 41 to 50 make up the largest proportion of the population with private health insurance coverage.23
Beneficiaries can access private care directly through their insurer’s network of hospitals and clinics, often with shorter wait times than in the public system.24
People working in the public sector are covered by three mutual funds financed through a mixture of government and member payroll contributions:25
MUFACE: covers civil servants
MUGEJU: covers judicial officials
ISFAS: covers members of the Spanish armed forces.
In 2023, about 78 percent of public sector employees chose private health care over public. People with private insurance often use public health care for emergency care and major surgeries but use private insurance for elective treatments and specialist visits.26
The Role of Government
The national government oversees, regulates, and coordinates the SNS. It provides public funding and supports initiatives such as the Recovery and Resilience Plan,which aims to modernize health care infrastructure and boost digital transformation. It also implements public health strategies to improve service delivery (see Health Care Innovation).27
The 17 autonomous communities manage planning, financing, and service provision. In some regions, private hospitals provide services under contracts with the public health system.28
“Each regional government manages its own health care services,” says Marta Villanueva Fernández, managing director at the IDIS Foundation. “This fact leads to some variation in how health care is delivered across the country, although core services and standards remain consistent nationwide.”
Each regional government manages its own health care services. This fact leads to some variation in how health care is delivered across the country, although core services and standards remain consistent nationwide.
Marta Villanueva Fernández
Managing Director
IDIS Foundation
The public institutions that are responsible for health care delivery are:29
The Ministry of Health: oversees SNS coordination to ensure cohesion, equity, and regulatory oversight
Autonomous communities: manage most public health resources, including hospitals, primary care centers, and emergency services
The Council of the National Health System: facilitates coordination between the Ministry of Health and autonomous communities
INGESA: manages health care in Ceuta and Melilla
Government-backed mutual funds(MUFACE, MUGEJU, and ISFAS): provide health care cover for civil servants, the armed forces, and the judiciary
Municipalities: handle public health initiatives, sanitation, and health promotion programs
The Agency for Medicines and Medical Devices: regulates pharmaceuticals and medical devices
The Spanish Network of Agencies for Health Technology Assessment and Services of the National Health System: evaluates new medical technologies before they are adopted by the SNS
Health Institute Carlos III: supports public health research, epidemiology, and health surveillance.
Integration and Care Coordination
There have been efforts to improve care coordination across primary, specialized, inpatient, community, and long-term care as well as to enhance patient outcomes, efficiency, and continuity of care.30
The SNS Digital Health Strategy (2021) aims to improve interoperability across regional health systems and facilitate cross-border care integration within the E.U. These efforts have strengthened communication between primary care providers, specialists, and hospitals and enabled remote monitoring and consultations (see Health Care Technology).31
Since 2019, some regions, including the Basque Country and Andalusia, have introduced organizations to improve transitions between primary and hospital care.32 Other initiatives include:33
The National System for the Assistance of Dependent People provides home care, telecare, and residential care for older adults and dependents.
Hospital-at-home programs were expanded to support early discharge and follow-up care. In Catalonia, the number of patients provided with home-based hospital care increased from 5,185 in 2015 to 8,086 in 2019.
Multidisciplinary teams were introduced in some autonomous communities to improve transitions between hospital and long-term care settings.
Primary care covers general, preventive, and chronic disease care and mental health support. General practitioners (GPs) act as gatekeepers to specialist services.
Secondary care includes hospital care, emergency care, and outpatient specialized care.
Tertiary care provides highly specialized treatments at major medical centers.
Public health care providers are paid based on a framework agreement with regional health services. These agreements define service volumes, budgets, and quality targets, such as improving patient safety. Compensation varies across autonomous communities but generally includes pay for performance, such as incentives for improving accessibility and chronic care management, with adjustments based on each region’s health priorities.35
Primary care payment approaches vary by region.Some, including Catalonia and the Basque Country, use risk-adjusted capitation models, while others, including Valencia, use public-private partnerships.36
Specialists in public hospitals are mostly paid through global budgets and capitation, but some receive additional fee-for-service payments for initiatives such as wait-list reductions. Hospitals receive funding based on discharges, case-mix weights (which measure the complexity and resource use of patient cases relative to the average), and a structure-related tariff (that covers fixed costs, such as staffing and facility management). Some procedures are reimbursed on a fee-for-service basis.37
Primary Care
GPs and staff nurses form the core of primary care teams.38 All residents are registered with a GP, who acts as a gatekeeper to specialized services.39
GPs are required to provide out-of-hours care (the number of required hours is not publicly available). In rural areas, doctors operate on a rota model, sharing patients and shifts, while urban areas have dedicated out-of-hours centers with telephone triage systems that direct patients to appropriate care.40
There are no data available for the number of primary care physicians practicing publicly versus privately.
The primary care system faces significant challenges. A 2023 study in Spain found that only 21.9 percent of patients were seen on the day they sought care or the day after seeking care from their family doctors.41 In addition, 26.1 percent of people opted for private providers.42
Workforce shortages contribute to the strain on services. In 2022, Spain had 95 GPs for every 100,000 people, below other E.U. countries, such as Germany (105) and the Netherlands (183) (see Physician Education and the Workforce).43
Since 2019, measures have been designed to strengthen the primary care system. The government has allocated more than EUR 750 million (USD 786 million) to upgrade infrastructure and acquire new equipment for primary care centers.44
Outpatient/Specialist Care
Secondary care in Spain encompasses specialized medical services provided in hospitals and outpatient clinics, typically after referral by a GP — although members of mutual funds can access specialists directly without referral.45
These services often complement ongoing primary care treatment, offering diagnostic, therapeutic, and rehabilitative services. However, patients often face long wait times for specialist care. As of 2023, the average wait time for a first specialist consultation was 87 days, 8 percent longer than in 2022. Neurology had the longest wait times for first appointments (118 days).46
As such, patients are turning to private providers (see Hospitals). In 2021, there were 2,260 outpatient specialist visits for every 1,000 people, of which about one in four (23%) were handled by private providers under contract with the public system.47
The number of specialist doctors has increased steadily, from 254 for every 100,000 people in 2017 to 283 for every 100,000 people in 2022. This number currently sits in the middle of other Western European countries, higher than the U.K. (236 per 100,000) but lower than Germany (350 per 100,000).48
There are no data available for the number of specialist physicians practicing publicly versus privately.
Physician Education and the Workforce
Spain has more doctors than the averages in Europe and high-income countries: 429 doctors for every 100,000 people in 2022, compared with 376 for Europe and 360 for high-income countries.49 As of 2024, there were 633 doctors per 100,000 people in Spain.50
But workforce shortages are a problem, especially in primary care. By 2028, Spain is expected to have 10,000 fewer GPs than it needs due to rising health care needs, an aging workforce (60% of GPs are over age 50), and difficult working conditions, including long hours, insufficient time with patients, and inadequate support for professional development.51
Health care access varies by region. In 2021, the number of doctors for every 1,000 people ranged from 2.3 in Andalusia to 3.8 in Asturias; 63 percent of active doctors were concentrated in just five of the 17 autonomous communities. The Balearic Islands and Castilla y Léon had even lower GP ratios (0.6 and 1.1, respectively, for every 1,000 people).52
Medical graduates are increasingly seeking opportunities abroad, including 12 percent of GPs. In 2020, 5,176 doctors trained in Spain were working overseas, and 2 percent of Spain’s GPs were practicing abroad in 2021.53
Temporary contracts contribute to job instability, limit career development, and cause high turnover rates. Between 2012 and 2020, the number of temporary contracts in the SNS rose from 28.5 to 41.9 percent. In 2022, the government launched reforms to curb these contracts and hired 80,000 health care professionals.54
In 2023, the Ministry of Health issued guidance to help identify hard-to-fill primary care roles — based on factors such as geographic isolation, high patient loads, or housing costs — and recommended incentives, such as additional pay, housing support, and professional development opportunities, to attract and retain primary health care professionals.55
The nursing shortage
Nursing shortages are even more severe. In 2021, Spain produced 23 nursing graduates for every 100,000 people, well below the E.U. (44.2) and OECD (42.8) averages.56 Primary care is particularly affected, with only one family and community nurse in training for every 100,000 people in 2022.57 In 2021, Spain also had fewer practicing nurses (630 for every 100,000 people, compared with 920 across the OECD) and a lower doctor-to-nurse ratio (1.4, compared with 2.5 across the OECD).58
Education
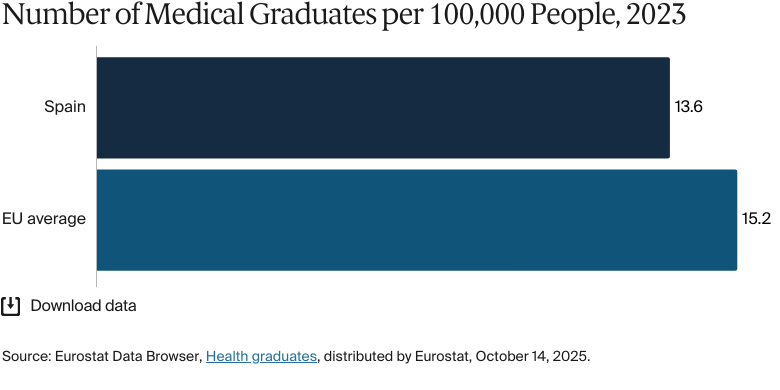
In 2023, there were 13.6 medical graduates for every 100,000 people in Spain, compared to 15.3 on average in the E.U.59
To expand the workforce, public universities added 706 spaces for medical students in the 2023–24 academic year, taking the total to 6,106 first-year places. This increase was backed by EUR 52 million (USD 56.5 million) in government funding.60 But the number of medical graduates is still below the E.U. average.61
Medical students in Spain attend a six-year curriculum and are eligible to practice medicine across the E.U. As of 2018, Spain had 42 medical schools (31 public and 11 private).62 Public university fees are determined by each autonomous community and are updated annually.63
In 2021–22, 224,080 international students were enrolled in higher education, but there is no specific information on medical students or on the proportion of the workforce that is recruited from overseas or chooses to work overseas.64
The government has also expanded internship training, with a 29 percent increase in positions from 2019 to 2024.65
Hospitals
BY THE NUMBERS
In 2025, there were 238 hospital beds per 100,000 people (compared with an average of 511 across the European Union in 2023).66
In 2024, there were 721 nurses per 100,000 people.67
In 2022, Spain had 751 hospitals: 331 public, 52 private, and 368 under mixed or alternative management models, such as public-private partnerships.68 Hospital density is low, with 16.4 hospitals for every one million people in 2021, significantly below the OECD average of 27.4 for every one million people.69
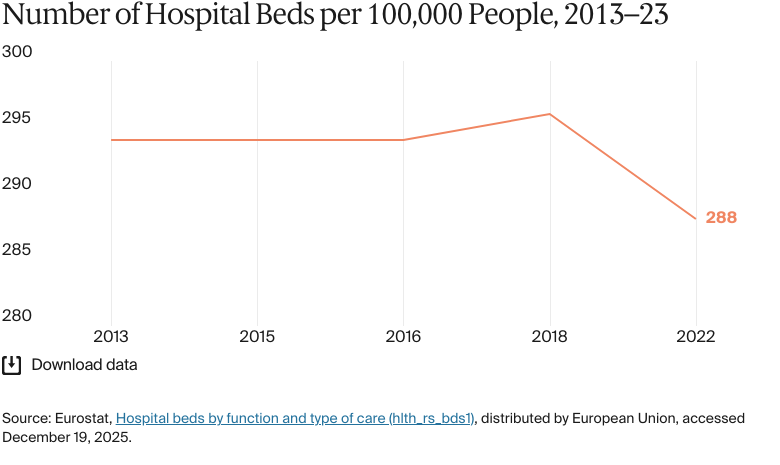
Bed capacity lags behind other E.U. countries: Spain had 291 beds for every 100,000 people in 2023, far fewer than Germany, for instance (755 for every 100,000).70 The number of hospital beds increases annually to match population growth. In 2023, there were 114,000 beds, equating to 236 for every 100,000 people. By 2025, there were 117,000 beds, but with population growth, the ratio remained stable at 238 for every 100,000.71
Spain has expanded long-term care services, but public hospitals remain the primary providers of complex and long-term treatments, leading to high bed occupancy rates and longer wait times.72 Staffing shortages, especially among nurses, strain hospital capacity (see Physician Education and the Workforce).
Long wait times are one of the main issues facing patients in the SNS. In 2025, the Ministry of Health reported an average wait time of 94 days for a hospital consultation and 121 days for a nonurgent surgery.73 As a result, many patients use private hospitals, where the average wait time for a first specialist consultation is between 9.8 and 16.5 days and for surgery is 24.1 days.74 In 2022, private hospitals handled 33.6 percent of first-time outpatient visits, compared with 28.3 percent in public hospitals.75
Mental Health Care
BY THE NUMBERS
There were nine psychiatrists per 100,000 people in 2020, the same as the average across high-income countries.
Mental health care is integrated into the SNS, covering diagnosis, treatment, and psychotherapy. Services are provided through a tiered system:76
Primary care handles early detection and follow-ups, with GPs referring patients to specialists as needed.
Outpatient care addresses addictions, child disorders, and specialized treatment.
Hospital care provides emergency and long-term treatment for severe cases.
Mental health issues have become increasingly prevalent. In 2019, about one in six people experienced mental health problems.77 By 2024, 59 percent of people considered mental health Spain’s most pressing health issue.78
The economic burden of depression and anxiety is rising. In 2021, spending on these conditions reached EUR 1.51 billion (USD 1.58 billion), a 15 percent increase from 2019.79 Spain is also one of the highest consumers of anti-anxiety medications in the E.U.80
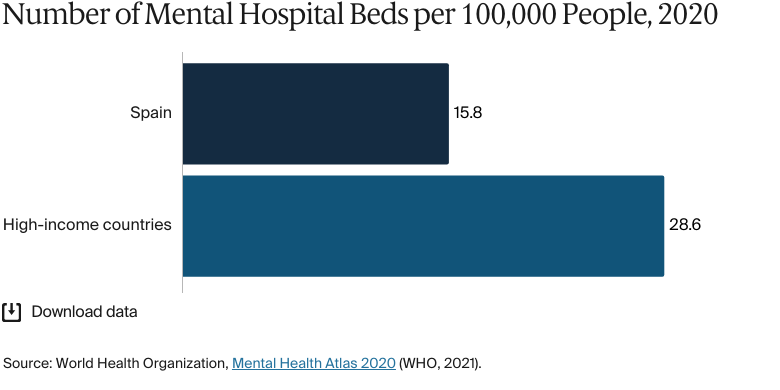
Mental hospital beds are in short supply, and occupancy rates are high. In 2020, there were 15.8 mental hospital beds for every 100,000 people, significantly below the average in high-income countries of 28.6.81 By 2022, bed occupancy rates in mental health hospitals had reached 82 percent, potentially delaying critical care for new patients.82
Staffing shortages exacerbate the problem. In 2022, mental health hospitals had just 18 nurses for every 100 beds, the lowest ratio across all hospital types (compared with 160.5 nurses for every 100 beds in general hospitals). With an average stay of 131.3 days per patient — compared with just six days in general hospitals — mental health facilities require more resources to provide adequate care.83 In 2022, there was only one mental health nurse in training for every 100,000 people (see Physician Education and the Workforce).84
The COVID-19 pandemic intensified the demand for mental health care and pushed it to the forefront of public health policy, leading to the Mental Health Strategy 2022–26, which prioritized community-based care, social inclusion, patients’ rights, and reducing stigma. In addition, the Mental Health Action Plan 2022–24 allocated EUR 100 million (USD 108.2 million) to training and awareness campaigns.85 Additional measures include:86
A national suicide prevention hotline
New leave allowance (introduced in 2023) for companions of individuals at imminent suicide risk
A rehabilitation program for doctors struggling with mental health or addiction, which connects them with professional support networks.
Long-Term Care and Social Support
By 2060, over 27 percent of seniors will be 85 or older, about 10 percentage points higher than in 2021. This will increase demand for long-term care services.87 To ease pressure on hospitals and residential facilities, the home care network has undergone expansion. Primary health care professionals have made 13 million home visits a year since 2023.88
Long-term care is managed regionally. The autonomous communities fund 64 percent, with the remainder funded by cost sharing (21%) and national government contributions (15%).89 Services, which cover home assistance, personal autonomy programs, and residential/nursing home care, are offered through a network of public, private, and nonprofit providers.90
The Dependency Act (2006) established the System for the Assistance of Dependent People (SAAD), which provides access to personal care, home support, and financial aid for caregivers. Eligibility and copayments are based on dependency level and income.91
By late 2022, SAAD was supporting 1.3 million people, with 70 percent receiving personal services and 30 percent receiving financial aid. Total SAAD spending reached EUR 10 billion (USD 10.9 billion), an average of EUR 8,321 (USD 9,037) per beneficiary.92
In 2024, the government allocated EUR 3.4 billion (USD 3.6 billion) to SAAD. In 2025, Dependency Act reforms aimed to expand benefits, widen eligibility, increase funding, and introduce anti-discrimination measures.93
Spain’s elderly care sector is largely privatized: only 25 percent of care home places are publicly owned, and some of these are under private management. About 34 percent of private facilities receive government subsidies to support lower-income residents.94
Hospital-based long-term care, meanwhile, is under strain. In 2022, medium- and long-term care hospitals had the highest bed occupancy rate (87%), and patients stayed for longer than a month, on average, limiting availability for new patients.95
Traditionally, there has been a reliance on family-based caregiving — mainly by women — but higher female workforce participation, declining informal care, and an aging population are now creating gaps in care.96
The 2022 Strategic Project for Economic Recovery and Transformation of the social and care economy was designed to address these problems by:97
Improving care quality and dignity
Distributing care responsibilities more evenly
Strengthening the public care system
Expanding services for those with moderate dependency
Reducing reliance on family caregivers and migrant workers.
Cost and Affordability
Health Care Spending Overview
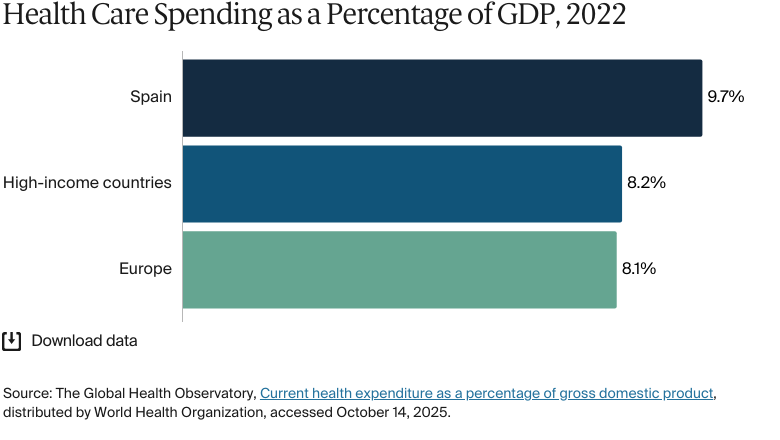
Health care spending has steadily increased. In 2022, health expenditure reached 10 percent of GDP, up from 8.9 percent in 2017. This is higher than the averages in high-income countries (8.2%) and across Europe (8.1%).98
Government figures from 2022 put total health spending at EUR 134 billion (USD 141 billion), up from EUR 110 billion (USD 127 billion) in 2018.99 But per capita spending is lower than in other Western European countries. In 2022, per capita health expenditure was USD 3,320, significantly below the regional average of USD 5,200.100
The largest contributor to health expenditure is public funding: 74 percent of spending in 2022, up from 70.3 percent in 2018.101
Pharmaceutical Spending
Pharmaceutical spending is a significant portion of total health care expenditure (15% in 2023).102 In 2015, total pharmaceutical expenditure was USD 491 per capita; by 2022, this had increased to USD 741 per capita.103 In 2023, Spain had the fourth-largest pharmaceutical market in Europe, generating EUR 32 billion (USD 37.1 billion) in revenue.104
Although the health care system is decentralized, medicine prices are set through a centralized process led by the Ministry of Health. A committee, including representatives from the autonomous communities, reviews and approves prices of prescription medicines before they go to market. The committee doesn’t set prices for drugs that aren’t reimbursed by the public system.105
Prices are evaluated based on local market comparisons, external reference pricing, and cost-effectiveness. Several discounts are applied to types of medicines and stages of development. For example, a standard 40 percent discount is applied to the first generic version of a medicine, and a 30 percent discount is applied to the first biosimilar version.106
Cost Sharing and Out-of-Pocket Spending
In 2023, out-of-pocket spending made up 21 percent of total health expenditure.107 Average household expenditure on health care rose from EUR 389 (USD 418) in 2015 to EUR 746 (USD 803) in 2022.108
Inpatient medication is covered by the SNS, but patients have a copayment for outpatient medication, depending on income. People earning more than EUR 100,000 (USD 108,606) a year pay 60 percent of the price, while those earning less than EUR 18,000 (USD 18,890) pay 40 percent.109 Copayments for orthoprosthetic devices also follow this structure.110 Retired public sector employees covered by one of the mutual funds contribute 30 percent.111
Some medications for long-term conditions have a reduced copayment, 10 percent of the price, with a maximum charge of EUR 4.24 (USD 4.6) per prescription item.112 Medicines provided in hospital outpatient settings for some conditions, including HIV/AIDS, are exempt from copayments.113
No one in Spain has been pushed below the poverty line because of health expenditure. This finding was consistent between the earliest available data from 1996 and the latest available data from 2019.114
How Are Costs Contained?
The decentralized structure of Spain’s health care system contributes to cost containment by allowing autonomous communities to manage planning, budgeting, and purchasing within defined funding allocations. This encourages more targeted and disciplined spending aligned with regional needs.
Some regions have introduced innovative approaches to improve efficiency. For example, Catalonia has piloted population-based contracts, and Navarre has implemented risk-stratification tools to identify patients with the greatest health needs so that services can be better targeted and coordinated.115
There are also fixed rules for how much wholesalers and pharmacies can add to the price of outpatient medications. Lower-priced medicines have percentage-based price margins; higher-priced ones have fixed price margins. Since 2000, pharmacies have had to return a portion of their earnings based on their annual sales of reimbursable medicines.116
Quality and Outcomes
Health Outcomes
BY THE NUMBERS
In 2021, life expectancy was 82.7 years (compared to 79.7 years on average for high-income countries in 2021).117
In 2021 life expectancy for women was 85.3 years (compared to 82.3 years on average for high-income countries in 2021).118
In 2021 life expectancy for men was 80 years (compared to 77.1 years on average for high-income countries in 2021).119
The avoidable mortality rate was 142 per 100,000 people in 2023.120
The top three causes of death in 2024 were:
Ischemic heart disease: 55 per 100,000 people
Bronchial and lung cancer: 48 per 100,000 people
Cerebrovascular disease: 47 per 100,000 people.121
The maternal mortality rate was 2.7 deaths per 100,000 live births in 2023 (compared with 11 on average in Europe in 2023).122
The infant mortality rate was 2.6 deaths per 1,000 live births in 2023 (compared with 6.6 on average across Europe).123
In 2021, the share of the population with mental health disorders was 19 percent (compared with 16% on average in high-income countries).124
In 2023, the suicide rate was 8 per 100,000 people, a lot lower than the average of 12 across high-income countries.125
Guns were responsible for 0.5 deaths in every 100,000 in Spain in 2023.126
In 2022, 16 percent of adults were affected by obesity.127
In 2021, average life expectancy was 82.7 years, above the 79.7-year average for high-income countries. There was a five-year difference between the life expectancies of men (80 years) and women (85.3 years).128
Avoidable mortality from preventable and treatable causes was on a downward trend from 2012 to 2019 but spiked in 2020 — most likely because of the COVID-19 pandemic — from 172.6 to 205.6 avoidable deaths for every 100,000. In 2021, it dropped slightly to 194.9 but remained above prepandemic levels. Despite this, Spain has one of the E.U.’s lowest avoidable mortality rates.129
In 2023, the maternal mortality rate in Spain was low (2.7 deaths for every 100,000 live births). This was under half of the average in Europe in 2023 (11.2) and well below the global average of 197.3.130
In 2023, 210,000 to 260,000 people had Alzheimer’s disease, heavily impacting families, which often act as informal caregivers. The disease also significantly impacts SNS resources; the average annual cost per patient, for instance, ranges from EUR 42,336 (USD 44,365) to EUR 70,445 (USD 73,820).131
In 2022, homelessness affected 60 people for every 100,000, significantly fewer than in much of Europe. In Germany, for instance, 310 people for every 100,000 were homeless in 2022.132
Addressing Health Inequities
Although the SNS provides broad coverage, people in the lowest-income quintile have more difficulties accessing health care. In 2024, 25.8 percent of the population was at risk of poverty or social exclusion.133
Health inequities affect cancer screenings and dental care in particular. In 2019, 49.2 percent of women ages 20 to 69 in the lowest income quintile underwent cervical cancer screening, compared with 65.3 percent in the highest quintile. In 2022, 4.6 percent of the population reported neglecting their dental care, exceeding the E.U. average of 3.4 percent. This was particularly pronounced among the lowest quintile group (10.5% vs. 0.8% in the highest quintile group).134
Following the World Health Assembly’s Global Action Plan on Oral Health (2023–2030), Spain is addressing disparities in dental care, aiming to expand coverage by 2030. The government is particularly focused on improving coverage for pregnant women, children, and people with disabilities.135
Since adopting the European Plan to Combat Cancer in 2021, Spain has expanded screening programs nationwide.136 In 2024, the government launched a cancer surveillance system to strengthen research and prevention programs across all autonomous communities.137 In 2023, it invested EUR 795 million (USD 834 million) in equipment for cancer treatment and diagnosis.138
Disparities in self-rated health exist between immigrants and native Spaniards, particularly among those residing in Spain for six to 15 years. The European Health Interview Survey, conducted in 2014 and 2020, shows that these disparities remain even after adjusting for factors such as age, gender, education, and health care use. The study suggests that poorer self-rated health among immigrants may be linked to structural disadvantages, including lower socioeconomic status, worse living and working conditions, exposure to discrimination, and limited access to health care services.139
Despite SNS coverage, homeless individuals and asylum seekers face significant barriers to accessing health care. The level of homelessness is one of the lowest in Europe, but life expectancy for the homeless population is 30 years shorter than the national average. These groups often struggle due to a lack of the necessary documentation, limited awareness of available health services, and limited coordination between health and social services.140
To address this, Spain introduced the National Strategy to Combat Homelessness 2023–30, which prioritizes better access to health care through housing initiatives, as well as better collaboration between health care, social services, and nongovernmental organizations.141 There is no recent information on health-related measures for asylum seekers and migrants.
The Roma community, which accounted for 2 percent of the population in 2020, faces lower life expectancy, higher rates of chronic diseases, poor nutrition, and low vaccination rates, largely due to persistent socioeconomic disadvantage, barriers to health care access, and systematic discrimination.142 Since 2003, the government has implemented a range of strategies to reduce health disparities, culminating in the National Strategy for Roma Equality, Inclusion, and Participation 2021–30.143
The LGBTQ+ community also experiences higher rates of mental health issues, as well as less access to services for preventing HIV/AIDS and testing for sexually transmitted infections. The Public Health Strategy 2022 is supposed to address this by:144
Training health professionals in LGBTQ+ health needs
Expanding mental health and crisis intervention programs
Strengthening sexual health prevention systems.
Innovation and Reform
Health Care Innovation
Public Health Strategy 2022
The Public Health Strategy 2022 aims to improve public health governance, expand disease prevention, address health inequities, and modernize services.
The State Centre for Public Health which is planned to enhance intersectoral collaboration by integrating health into broader policies (for example, in education) to encourage a “health in all policies” approach.
The State Public Health Surveillance Network will provide real-time data to enable faster detection of and responses to public health threats.
Health Technology Assessment
The government is developing a health technology assessment process to streamline drug approvals and funding decisions. This process aims to increase transparency, improve cost control, encourage innovation, and ensure fair competition between brand-name and generic drugs.146
Health Care Technology
Digital Health Strategy
The Digital Health Strategy 2021–26 aims to improve health care accessibility and innovation through telecare, digital health records, and data-driven decision-making.147 By 2022, one result was the expansion of the My Citizen Folder (Mi Carpeta Ciudadana) app, which gives users streamlined access to public services, including digital health records. At that time, the app had over 1.4 million downloads and 1.9 million users, with an update that enabled access to digital medical histories from the SNS.148
To expand remote care access, particularly in rural areas, Spain is investing in telecare services. Government figures from February 2025 reported 87 million teleconsultations in primary care.149 Another important initiative is the creation of a fully interoperable digital health record to improve nationwide access to patient data. Part of this is the National Health Data Space, which is designed to use artificial intelligence and big data to enhance research and decision-making.150
Between 2021 and 2023, the government allocated EUR 800 million (USD 840 million) to support these efforts, including personalized health care initiatives. An example of personalized care is the Únicas Network, which is designed to improve care for rare children’s diseases through collaboration, research, and data sharing across health institutions in Spain and Europe.151
Electronic Health Records
Nationwide implementation of electronic health records has improved data accessibility, but there are challenges.152 A 2022 Ministry of Health study found that only 28.5 percent of people had accessed their electronic records, and 31.5 percent were unaware of their existence.153 This could be due to fragmented data, GDPR-related challenges, or a lack of coordination across different sectors.154
Some regions have made significant progress. Aragón, for instance, has developed a comprehensive data lake by integrating hospital, emergency care, laboratory, and prescription data into a single system.155
Private Sector Initiatives
Interoperability efforts also extend to the private sector. For example, the miHC project from the IDIS Foundation (a private health care advocacy group) is an interoperability platform designed to facilitate medical record exchange in private health care. “The goal is for patients to have access to their own medical records and to be able to share this information with professionals, regardless of the health care center,” says Fernández. “It’s a major step in creating a single European health data space."
This content was produced by FT Longitude, the specialist research and content marketing division of the Financial Times Group, on behalf of the Commonwealth Fund. Research and content for the Commonwealth Fund country profiles were collected by FT Longitude between February and December 2025.
This profile reflects data as of January 2026. New or updated information may have become available since its release.
Organisation for Economic Co-operation and Development, Spain: Country Health Profile. https://www.oecd.org/en/publications/2023/12/spain-country-health-profile-2023_727a7995.html↩
Organisation for Economic Co-operation and Development, Spain: Country Health Profile; Bernal-Delgado et al., “Health system review.”
↩
28
Organisation for Economic Co-operation and Development, Spain: Country Health Profile; Bernal-Delgado et al., “Health system review.”
↩
29
Organisation for Economic Co-operation and Development, Spain: Country Health Profile; Bernal-Delgado et al., “Health system review.”
↩
30
Organisation for Economic Co-operation and Development, Spain: Country Health Profile; Bernal-Delgado et al., “Health system review.”
↩
31
Organisation for Economic Co-operation and Development, Spain: Country Health Profile; Bernal-Delgado et al., “Health system review.”
↩
32
Organisation for Economic Co-operation and Development, Spain: Country Health Profile; Bernal-Delgado et al., “Health system review.”
↩
33
Organisation for Economic Co-operation and Development, Spain: Country Health Profile; Bernal-Delgado et al., “Health system review”; Rubèn González-Colom et al., “Five years of hospital at home adoption in Catalonia: impact, challenges, and proposals for quality assurance.” BMC Health Services Research 24 (February 1, 2024):154, https://doi.org/10.1186/s12913-024-10603-1.
↩
34
“Healthcare in Spain: All You Need to Know in 2026” Global Citizen Solutions, 2026, https://www.globalcitizensolutions.com/healthcare-in-spain/; Bernal-Delgado et al., “Health system review.”↩
Caroline Berchet and Carol Nader, “The organisation of out-of-hours primary care in OECD countries.” OECD Health Working Papers, September 21, 2016, https://doi.org/10.1787/5jlr3czbqw23-en.
↩
National Institute of Statistics, “Health Professional Statistics.”
↩
51
Sara Calderón-Larrañaga et al., “What can we learn from general practitioners who left Spain? A mixed methods international study.” Human Resources for Health 22 (January 23, 2024):9, https://doi.org/10.1186/s12960-023-00888-4.
↩
52
Katarzyna Dubas-Jakóbczyk et al., “Medical deserts in Spain—Insights from an international project.” The International Journal of Health Planning and Management 39, no. 3 (February 15, 2024):708–21, https://onlinelibrary.wiley.com/doi/full/10.1002/hpm.3782.
↩
53
Calderón-Larrañaga et al., “Practitioners who left Spain.
↩
Eurostat Data Browser, Health graduates. Calculated using population data from World Bank Open Data Population, total — Spain, distributed by World Bank Group, accessed February 21, 2025, https://data.worldbank.org/indicator/SP.POP.TOTL?locations=ES.
↩
Spain’s National Health System Information System, Key Data. Calculated using population data from National Institute of Statistics, “CPS: Provisional Data.”; Eurostat Data Browser, Hospital beds by function and type of care.
↩
67
National Institute of Statistics, “Health Professional Statistics.”
↩
68
Ministry of Health, Hospital Statistics; Bernal-Delgado et al., “Health system review.”
↩
Spain’s National Health System Information System, Key Data. Calculated using population data from National Institute of Statistics, “CPS :Provisional Data.”
↩
Luz M Peña-Longobardo et al., “The Spanish long-term care system in transition: Ten years since the 2006 Dependency Act.” Health Policy 120, no. 10 (October 2016):1177–82, https://pubmed.ncbi.nlm.nih.gov/27667653/; Bernal-Delgado et al., “Health system review.”
↩
Antía Pérez-Caramés, “Recent developments in long-term care in Spain: challenges and competing discourses amidst the global pandemic,” in Politicising and Gendering Care for Older People, edited by Anca Dohotariu et al. (Manchester University Press, 2024), 81–99, https://www.manchesterhive.com/display/9781526176004/9781526176004.00010.xml.
↩
“Suicide Rate by Country 2026”,World Population Review, accessed January 21, 2026, https://worldpopulationreview.com/country-rankings/suicide-rate-by-country
↩
126
Institute for Health Metrics and Evaluation, GBD Compare, distributed by IHME, 2023, https://vizhub.healthdata.org/gbd-compare/. Overall firearm mortality is an aggregate of physical violence by firearm, self-harm by firearm, and unintentional injuries by firearm.
↩
Laura Gómez Maldonado et al., “Cost of patients with Alzheimer’s disease in Spain according to disease severity.” PharmacoEconomics Open 8, no. 1 (November 15, 2023):103–14, https://pmc.ncbi.nlm.nih.gov/articles/PMC10781927/#Sec10.
↩
Explore how countries compare on key health system characteristics including health care coverage and spending, the health workforce, health outcomes, and more.