Background and History
The Philippines’ health care system has evolved over centuries, shaped by colonial rule and political change. Institutional development began with the creation of the Department of Health and Public Welfare in 1939, followed by the Department of Health in 1947, which expanded basic health services under the Rural Health Act of 1954. Subsequent reorganizations reflected shifts in government structure following the declaration of martial law in 1972 — from the change to the Ministry of Health in 1978, following the adoption of a parliamentary form of government, to its reestablishment as the Department of Health in 1986, following the People Power Revolution and a shift back to a presidential government.
In 1991, the Local Government Code of the Philippines decentralized the delivery of health services and gave local government units (LGUs) autonomy over, and responsibility for, local health care delivery. The National Health Insurance Act of 1995 created a system of social health insurance known as the Philippine Health Insurance Corporation (PhilHealth).
Subsequent reforms have included the launch of the 1999 Health Sector Reform Agenda to target systemic inefficiencies, such as fragmented service delivery, inequitable access to care, weak regulation, and underfunded local health facilities, and the FOURmula One for Health framework in 2005 to implement new strategies for health financing, regulation, service delivery, and governance.
In 2010, the government launched the universal health care (UHC) policy (Kalusugan Pangkalahatan), which focused on increasing PhilHealth membership and improving government health facilities through the Health Facilities Enhancement Program. UHC expanded health care coverage through PhilHealth, upgraded thousands of health facilities, deployed more than 23,000 health professionals, and mobilized community health teams — all of which improved service availability, expanded access to outpatient and inpatient care, and strengthened financial protections. These actions were followed by the enactment of the UHC Act in 2019, which guaranteed access to comprehensive services, regulated copayments to improve financial protection, and combined fragmented local health systems into province- and city-wide networks.
The Role of Public Health Insurance
The UHC policy strengthened PhilHealth’s role by automatically covering citizens through the National Health Insurance Program, regardless of their ability to pay premiums. The UHC also ensures that citizens are automatically enrolled in an essential health benefits package consisting of preventive, curative, rehabilitative, and palliative services, with no copayments for basic care in public hospitals and fixed copayments for higher-level services.
Although the National Health Insurance Program purports to provide coverage for all Filipinos, in reality, the government fails to enroll significant segments of the population — especially Indigenous communities (see Addressing Health Inequities).
As of June 30, 2024, PhilHealth had enrolled 83 percent of the population.
Services Covered by Public Health Insurance
The following services are covered under public health care:
- Preventive care
- Inpatient care
- Outpatient care
- Maternity care
- Primary care
- Pharmaceuticals
- Dental care
- Eye care
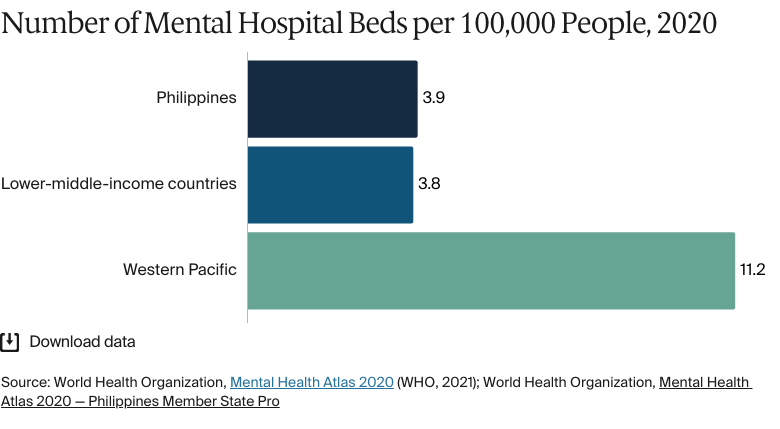
- Mental health care
- Palliative care
- Long-term care
- Rehabilitative care
- Home visits
- Assistive devices.
PhilHealth members are classified as either direct contributors (those who pay premiums, such as employees and pensioners) or indirect contributors (those whose premiums are paid for by the government). As of 2025, the contribution rate for direct contributors is 5 percent of income (to be equally shared by employer and employee). Employees who earn under PHP 10,000 (USD 175) a month pay a fixed premium of PHP 500 (USD 9), while the contribution of those who earn more than PHP 100,000 (USD 1,750) a month is capped at PHP 5,000 (USD 87).
In 2024, PhilHealth increased reimbursement rates for nearly all its case rate packages by 80 percent, backed by reserve funds totaling PHP 600 billion (USD 10.4 billion). The goal was to eradicate financial burdens for its members and facilitate timely access to essential medical services.
Safety Nets
The UHC Act automatically enrolls all Philippine citizens under the National Health Insurance Program through PhilHealth, which includes a comprehensive range of health services.
These systems of health financing are complemented by social protection programs. The Pantawid Pamilyang Pilipino Program, for instance, is a conditional cash transfer program for low-income families, with assistance tied to meeting such requirements as keeping children in school and attending regular health check-ups. The Department of Health assists poorer patients through the Medical Assistance Program, which provides necessary medicines free of charge in government hospitals, and the Z Benefit Packages, which pay for high-cost treatments for severe or major illnesses.
Another safety net, the Medical Assistance to Indigent and Financially Incapacitated Patients Program, provides financial aid to people with no income, those with insufficient income to meet their family’s needs, and those suffering from conditions that require expensive treatment they can’t afford. The level of aid is based on individual need.
The Role of Private Health Insurance
Private health insurance serves as a supplement to PhilHealth. In 2022, 39 percent of the population was covered by health insurance other than PhilHealth, and private insurance plans made up 13 percent of health spending in 2024.
The most common type of private insurance is provided by health maintenance organizations (HMOs) operating on a prepaid basis. Policies typically include consultations, hospitalization, outpatient services, and preventive care at hospitals in each HMO’s network. Annual premiums range from PHP 5,000 (USD 88) to PHP 20,000 (USD 351), depending on the benefits. Most HMOs in the Philippines set their own annual benefit limits, known as maximum benefit limits. Some premium HMO plans offer up to PHP 5,000,000 for hospitalization and PHP 100,000 for outpatient services per year.
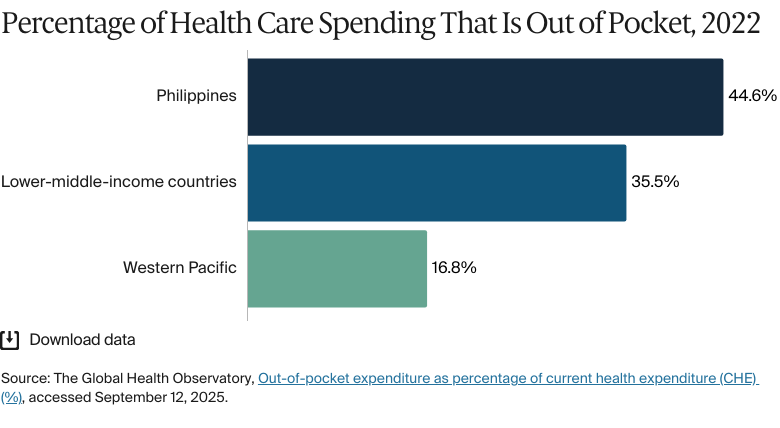
Many Filipinos enroll in HMOs to supplement PhilHealth, which only partially covers hospital bills and certain procedures, leaving patients with high out-of-pocket costs. HMOs offer cashless access: patients simply present their HMO card at accredited hospitals, and the provider charges the HMO directly. HMOs are commonly offered by employers as a benefit, making them a convenient option.
The Role of Government
The Philippine government plays an active role in regulating and delivering health services and promoting national and local collaboration.
At the national level, the Department of Health is the lead agency that sets policy, conducts regulatory supervision, sets standards, and carries out planning. It comprises 18 central bureaus and 17 regional health offices, which implement various national public health programs, such as immunization, disease control, and emergency health services, and work closely with LGUs. The Department of Health also supervises government-owned specialty and regional hospitals, licenses health facilities through the Health Facilities and Services Regulatory Bureau, and regulates health products through the Food and Drug Administration. PhilHealth automatically accredits all facilities accredited by a Department of Health regional office.
Health service delivery is mainly carried out at the local level. LGUs comprising provinces, cities, municipalities, and villages (barangays) are responsible for managing primary- and secondary-level health facilities. District and provincial hospitals are managed by provincial governments, while Rural Health Units and barangay health stations are under the jurisdiction of municipal governments. Governors or mayors lead Local Health Boards, which have representatives from the Department of Health, in overseeing health planning and service integration in communities.
Following earlier decentralization under the Local Government Code, which fragmented the public health system and led to uneven service delivery, the 2018 Mandanas-Garcia ruling increased LGUs’ funding from national taxes. This was followed by a 2021 executive order that mandated full devolution, making LGUs fully responsible for both funding and delivering health services using their expanded budgets.
Integration and Care Coordination
There have been significant steps to promote integration and care coordination, particularly at the primary care level. The UHC Act expanded PhilHealth’s primary care benefits with the Konsultasyong Sulit at Tama (Konsulta) package, which streamlines a range of services — including preventive, promotive, diagnostic, and rehabilitative care — through a unified primary care platform (see Primary Care).
The Department of Health has issued multiple policies guiding the integration of local health systems into province- and city-wide health systems to improve coordination, efficiency, and accountability. It establishes health care provider networks — groups of hospitals, clinics, and primary care providers working together to deliver continuous care. The initiative is monitored through frameworks that track LGUs’ progress in integrating their health services. Overall, it aims to ensure more equitable access to primary and specialized care, reduce fragmentation, and strengthen the country’s move toward universal health coverage.
The Malasakit Centers, established in 2019, are situated in government hospitals to streamline access to medical and financial assistance for low-income Filipinos. Bringing together the Department of Health, the Department of Social Welfare and Development, and PhilHealth in one place, these centers help qualified patients cover hospitalization, medicines, diagnostics, and transportation.
Overview of the Delivery System
The health system is organized into three service levels:
- Primary care is delivered via barangay health stations, Rural Health Units, and community clinics. It focuses on prevention, health promotion, early diagnosis, and the treatment of common diseases.
- Secondary care is provided by district and provincial hospitals. It includes specialized care and treatment that’s beyond the capacity of primary care providers, such as maternal health services, inpatient care, and basic surgery.
- Tertiary care is provided by specialized and regional hospitals, including government corporate hospitals. Tertiary facilities offer advanced diagnostic, therapeutic, and rehabilitation services for complex and advanced disease conditions.
The traditional fee-for-service payment system began to give way to a case-based system in 2011, when PhilHealth launched 23 case rates covering common conditions and procedures. In 2014, the All Case Rates system was implemented nationally. It bases all inpatient service reimbursements on fixed, standard rates to simplify claims processing, increase certainty, and reduce overutilization of services.
Primary Care
In the Philippines’ mixed health system, primary care is delivered through public facilities and private providers. Public primary care is delivered mainly through Rural Health Units and barangay health stations managed by LGUs.
Konsulta, launched in 2020 and scaled nationally by mid-2021, is a primary care package available to all PhilHealth-registered members. Designed to strengthen access, it focuses on basic curative and preventive services, offering annual check-ups, selected diagnostics, and essential medicines. As of 2024, Konsulta’s capitation rate increased to PHP 1,700 (USD 30) per registered beneficiary annually for both public and private providers. Payment is split into two tranches: 40 percent on registration and first patient encounter and 60 percent based on performance metrics. While public providers deliver services at no cost, private providers are permitted to charge a copayment of up to PHP 900 (USD 16) per beneficiary annually.
The Barangay Health Worker program strengthens primary health care at the community level through trained volunteers who provide basic services and health education. Complementing this, general practitioners (GPs) provide primary health care by diagnosing common conditions, performing minor procedures, and referring complex cases — often through private practice or as salaried staff in health facilities.
As of 2024, there were about 19.5 GPs for every 100,000 people. There are no data available on the number of GPs practicing publicly versus privately, nor are there regional GP data.
As of 2021, there were about 3,900 primary care facilities, including about 2,590 Rural Health Units. However, nearly half the population found it difficult to access them, being unable to reach one within 30 minutes.
Under the UHC Act, every citizen is required to register with a primary care provider of their choosing. However, the registration process has faced operational challenges, such as a lack of facility accreditation and confusion about procedures. By 2022, only 8.5 percent of PhilHealth members were registered with accredited primary care providers, highlighting implementation gaps.
Outpatient/Specialist Care
The decentralized health care delivery system has led to overlapping referral patterns, with district hospitals, rather than primary care facilities, sometimes serving as the first point of care. This has resulted in overcrowded district hospitals, underutilized primary care facilities, and the redirection of patients back to their local barangays.
Disparities in access to specialist and outpatient services are significant, particularly for families in remote and underserved areas. These households experience higher disease burdens and a greater need for outpatient care but face considerable barriers to accessing these services, leading to lower benefit utilization and higher out-of-pocket spending. (see Addressing Health Inequities)
As of 2024, there were 21.4 specialists for every 100,000 people. There are no recent data available on the number of medical specialists practicing publicly versus privately, nor are there regional specialist data available.
Physician Education and the Workforce
The medical education system combines academics with extensive clinical training. Aspiring doctors take the National Medical Admission Test.
The core Doctor of Medicine program takes four years, after which graduates must pass the Physician Licensure Examination. Candidates then complete a mandatory one-year postgraduate internship to gain practical experience. Those pursuing specialization proceed to residency training, which lasts three to six years, depending on the chosen field. Tuition fees for medical degreed at state universities in the Philippines are paid in full by the government.
With 64 authorized medical schools and English as the main teaching language, the Philippines is emerging as a medical education hub in Asia. To support this, funding under the Doktor Para sa Bayan Act aims to increase the number of physicians by providing full medical scholarships, exam review support, and higher allowances for students.
Still, the Philippines faces a critical health care workforce crisis due to the migration of skilled medical professionals to countries that offer better pay and working conditions. Senior staff, in particular, are increasingly choosing to work abroad. This migration has led to significant staffing shortages at both public and private hospitals, longer wait times, reduced hospital services, and overburdened staff.
Entry-level nurses in private hospitals earn between PHP 15,000 (USD 263) and PHP 25,000 (USD 438) a month, leading many to leave the system. As of 2021, about one-third of the country’s 900,000 registered nurses were working abroad, while over 290,000 licensed nurses had shifted to non-nursing careers domestically. By 2023, only 170,000 nurses were active in public and private health care facilities.
In response, the government has introduced several initiatives to expand local access to medical education and strengthen the health care workforce. There has been an increase in the number of new medical school programs approved by the Commission on Higher Education, particularly in underserved regions. In addition, the Department of Migrant Workers has proposed a scholarship fund for aspiring nurses, to be funded by countries recruiting Philippines-educated nurses. (As of July 2025, there had been no formal updates on this.)
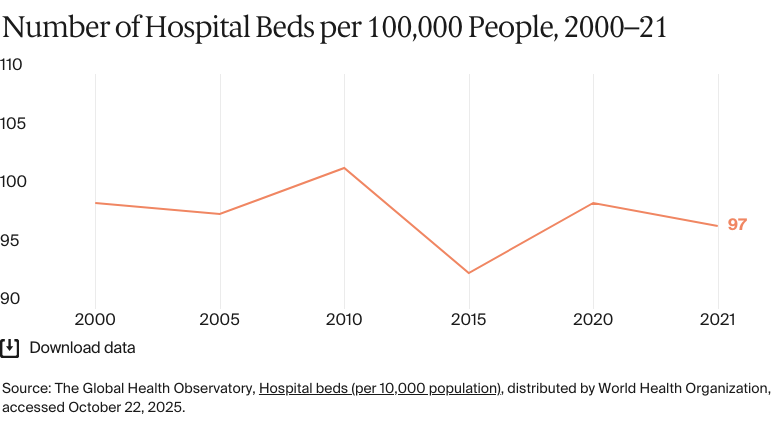
Hospitals