With hospital financing largely tailored to urban contexts, a growing number of rural hospitals are closing their doors, leaving many rural residents without a place to go for care. Since 2005, nearly 200 rural hospitals have completely or partially closed, and over 400 — more than 20 percent of rural hospitals — are at risk of closure. Even the hospitals that manage to stay open are cutting critical services to make ends meet. Between 2014 and 2023, for instance, 424 rural hospitals stopped offering chemotherapy services, forcing cancer patients and their families to travel farther to access needed care.
Beyond creating barriers for patients, hospital closures worsen workforce shortages as physicians leave the community for employment. Other types of care facilities, like community health centers, are left to pick up the slack, but they can’t offer the same services as a hospital and may face their own financial challenges. And as demand for care rises in the area, so do prices at remaining hospitals.
Why are rural hospitals losing money?
Health care clinicians and health systems in the United States are largely paid based on how many services they deliver. This is particularly challenging for rural areas, which have smaller populations and fewer patients, resulting in lower demand for services. As a result, rural hospitals often cannot generate enough revenue to pay for their fixed, overhead costs by providing services. While urban hospitals tend to have higher operating costs, they have the patient volume to afford it. A higher proportion of rural hospital revenue, on the other hand, is spent on staying afloat rather than investing in improvements to care and infrastructure.
Maternity care offers a useful case study. Though access to maternal health services is critical for safe pregnancy and delivery, low numbers of rural births have forced the closure of maternity wards. In 2024, roughly a third of U.S. counties didn’t have a single obstetric provider or birthing facility. To provide maternity care, rural hospitals must employ specialized staff and have beds and equipment available year-round, but they are only paid when a delivery actually occurs. The low frequency of these deliveries means reimbursements often fail to offset the fixed costs of making these services available.
When facing repeated shortfalls, rural hospitals have three choices: lose revenue, which can put them at risk of closure; rely on payment from other services to subsidize operating costs for maternity care; or stop providing this care altogether. They are increasingly choosing the third option, and rural families are paying the price.
Complicating matters, a larger share of rural than urban residents are insured by public payers such as Medicare and Medicaid, which typically reimburse less for services than private payers. Within Medicare, an increasingly large share of rural patients are enrolled in Medicare Advantage plans, which tend to have lower provider payment rates than traditional Medicare and higher rates of claims denials. Fewer patients and lower reimbursement rates mean nearly half of rural hospitals operate on negative or close-to-negative margins.
How can rural hospitals bolster their finances?
Over time, various congressional and federal policies aimed at bolstering rural hospital financing have created a patchwork of payment mechanisms.
Medicare, the largest payer for rural health care services, predominantly pays for hospital care through two mechanisms: the inpatient and outpatient prospective payment systems, known as IPPS and OPPS. Under IPPS, Medicare pays a predetermined rate per hospital stay, which should also cover operating and capital costs. Under OPPS, Medicare similarly pays a predetermined rate for each episode of care based on the type and complexity of services delivered. Medicare applies geographic adjustments to IPPS and OPPS payments to account for differences in volume and operating costs in rural versus urban settings.
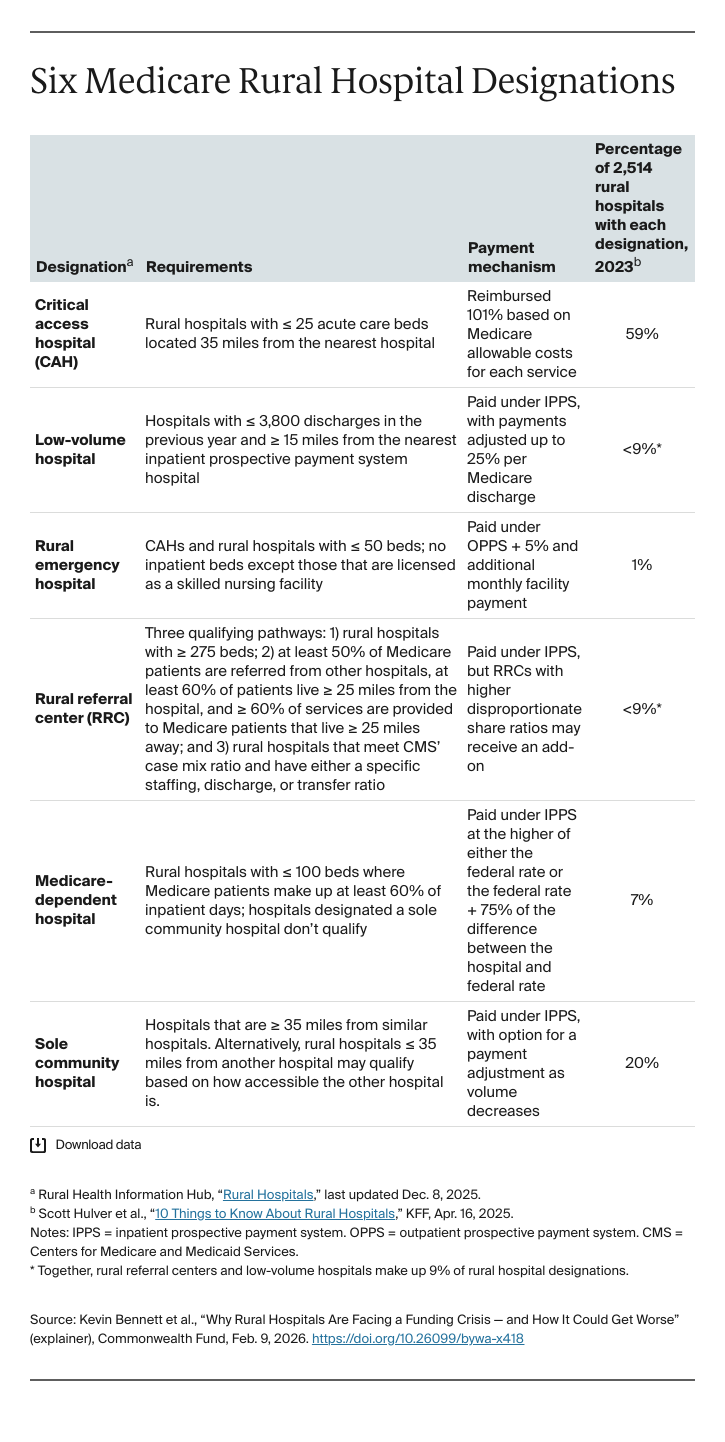
Medicare also has several programs that build on IPPS and OPPS by offering rural hospitals enhanced payments and/or flexibility in regulatory requirements. To qualify, a rural hospital must have low patient volume, have few hospital beds, or be the only hospital within a geographic area, making it critical for maintaining patient access (see the table describing six programs). Nearly all rural hospitals receive funding through one of these three designations. Over half of rural hospitals are designated critical access hospitals.
Many rural hospitals also benefit from disproportionate share hospital payment programs in Medicare and Medicaid, which help cover some uncompensated care costs for hospitals that serve a high proportion of low-income patients, untied to geography.
Additionally, rural hospitals may receive tax incentives, charitable donations, and private investments through venture capital or private equity. Notably, there are some concerns regarding private investments in hospitals, regardless of geography, with evidence showing it has led to hospital consolidation, closures, and higher consumer prices. Findings are mixed regarding their impact on quality of care.
Finally, the Rural Health Transformation Program, included in the 2025 budget bill H.R. 1, provides $50 billion in funding to states. The Centers for Medicare and Medicaid Services (CMS) has stipulated that no more than 15 percent of funds can be used on hospitals or patient care.
While these programs are meant to augment insurer payments to hospitals, they do not address the impact that low visit volume has on rural hospitals. Without a stable, baseline level of funding, rural hospitals must find alternative sources of funding to maintain their operations.
How has Medicaid expansion impacted rural hospital financing?
The Affordable Care Act’s (ACA) expansion of Medicaid eligibility made coverage available to nearly all low-income adults in the 41 states (including the District of Columbia) that opted in. For rural residents in these states, it’s meant that a higher proportion of patient visits are reimbursed, because more rural residents are now insured, leading to increased revenue for hospitals. In the first two years of expansion, Medicaid revenue shares for rural hospitals rose an average of 33 percent — equivalent to about $2 million more in revenue — while uncompensated care costs fell 43 percent. Medicaid expansion is associated with positive operating margins and lower probability of hospital closure. While the benefits of expansion apply to both rural and urban hospitals, rural hospitals experience greater financial gains.
What impact might congressional policy changes have on rural hospital financing?
The 2025 budget bill, H.R. 1, includes several provisions focused on Medicaid expansion states that are expected to erode the financial stability of rural hospitals. Medicaid spending in rural areas is expected to decrease by $137 billion over the next 10 years, with expansion states seeing the largest reductions. Rural hospitals’ Medicaid revenue could drop by as much as 9.6 percent on average, while uncompensated costs could increase by 35.4 percent. Key changes include:
- Medicaid beneficiaries who became eligible through the expansion are now required to regularly verify their work status to stay enrolled, and states will need to redetermine their eligibility every six months rather than 12 months. These changes are expected to cause 1.5 million rural Medicaid beneficiaries to lose coverage.
- A new cap on state-directed payments is expected to accelerate hospital closures. It limits the capacity of state Medicaid programs to provide enhanced payments to rural hospitals, helping to offset low Medicaid reimbursement rates.
In addition to H.R. 1, enhanced premium tax credits expired at the end of 2025. Without these credits, which subsidize the cost of ACA marketplace health insurance plans, fewer people will be able to afford coverage, and rural hospitals could lose an additional $1.6 billion in patient revenue.