Abstract
- Issue: Accessible, comprehensive, continuous, and coordinated primary care benefits patients, yet is not supported well by Medicare’s current payment system.
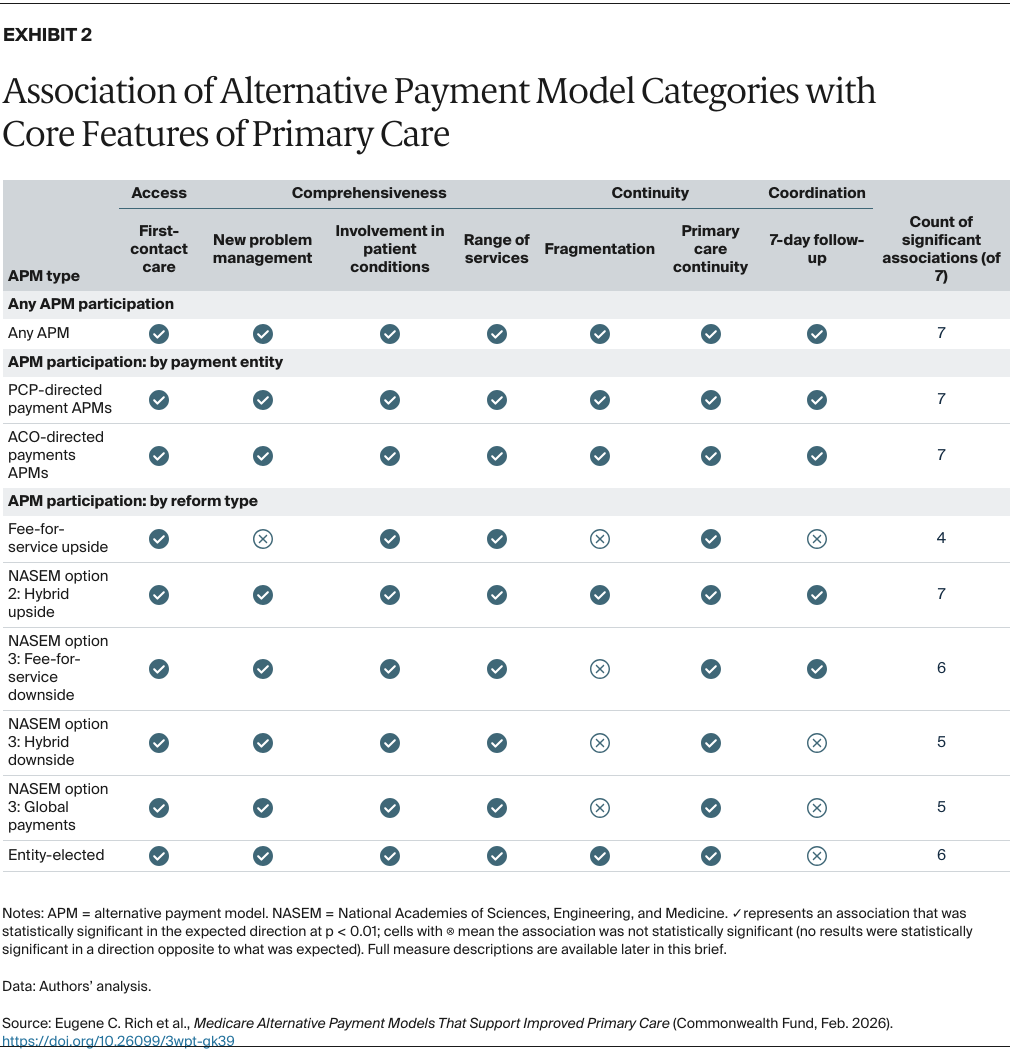
- Goals: To identify which types of alternative payment models (APMs) being tested in traditional Medicare have been associated with improvements in the four core primary care features of access, comprehensiveness, continuity, and coordination.
- Methods: We conducted difference-in-differences analyses of claims data to identify which APM types were associated with improvements in measures of the key features of primary care.
- Key Findings: APM participation was associated with improvements in at least one measure for each key feature of primary care. APMs that pay primary care practices (rather than larger entities) achieved greater improvements for measures of access and comprehensiveness. Primary care practices in “hybrid” APMs without financial risk improved on all measures, while findings were mixed for other reform models.
- Conclusion: Disentangling primary care practices’ finances and rewards from those of other providers and larger organizations may be essential to future success in restoring primary care to its core role in health care delivery. Payment models that provide hybrid payments to these practices without adding financial risk appear effective at supporting the essential features of primary care.
Introduction
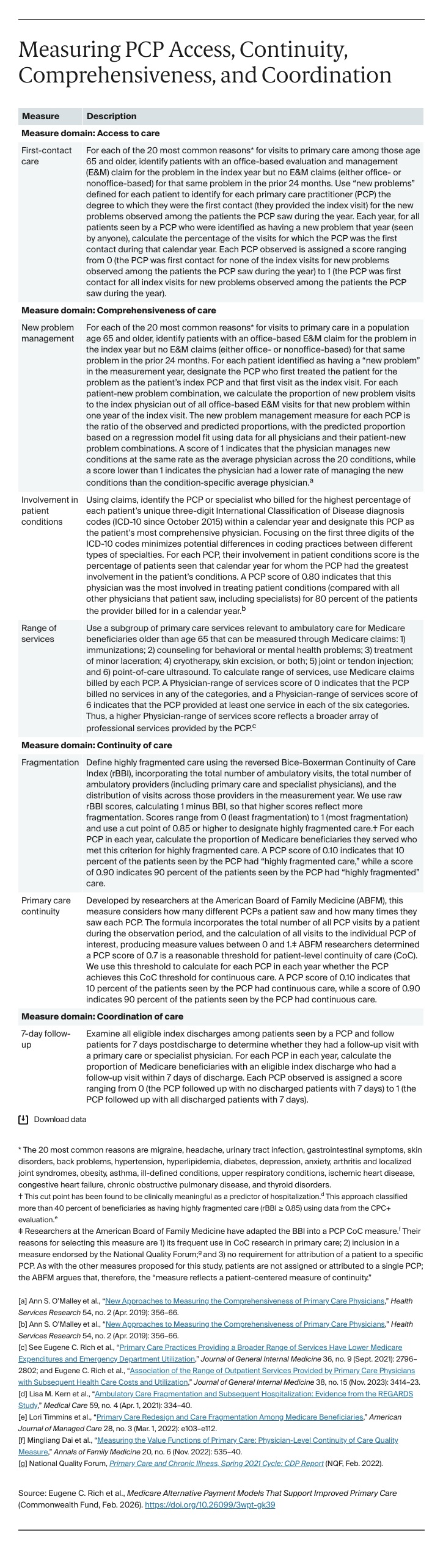
Primary care is critical for population health, health equity, and the overall efficiency of the health care system.1 It also has been consistently associated with improved life expectancy and reduced health care disparities. The four defining features of high-functioning primary care are:
- accessibility
- comprehensive care for most patient problems
- continuity of care over time
- coordination of care with the broader health care delivery system.2
Though extensive research has demonstrated the value to patients and the wider community when primary care practitioners (PCPs) deliver care defined by these key elements, they are often lacking in the United States.3 Compared to other high-income countries, U.S. patients are less likely to have a usual source of care, after-hours access to primary care, or a longstanding relationship with a provider of comprehensive primary care.4 One reason is Medicare’s physician fee schedule, which does not adequately incentivize primary care practices to provide accessible, comprehensive, continuous, or coordinated care.5 For example, fee schedule payments do not support the additional costs of providing care outside regular business hours, which can limit accessibility for people with caregiving responsibilities, multiple jobs, or jobs with irregular hours.6 PCPs are also providing less comprehensive care, increasingly referring patients to specialists for in-depth management after documenting their concerns.7
While the Medicare fee schedule recently added codes for time spent coordinating care outside the face-to-face visit, barriers such as administrative costs to the practices and copayments for patients mean few PCPs utilize them.8 PCP continuity is also inadequately supported by current fee-for-service payments: practices that rely on revenue from visits lose money when there are unused appointment slots held to accommodate last-minute visits from established patients.9
Recognizing the limitations of the Medicare fee schedule in supporting primary care, the Centers for Medicare and Medicaid Services (CMS) has designed and tested alternative payment models (APMs) for primary care providers serving patients in the traditional Medicare program. We recently assessed 14 of these APMs to evaluate whether they improve delivery of the four defining features of primary care.10
To group these models and better understand which reforms might be associated with improvements, we adapted a framework advanced by the National Academies of Sciences, Engineering, and Medicine (NASEM) in its 2021 consensus study.11 In this issue brief, we use our findings to explore lessons learned for the design of payment models to enhance the provision of the core features of primary care.
Key Findings
Options for Improving Payment for Primary Care
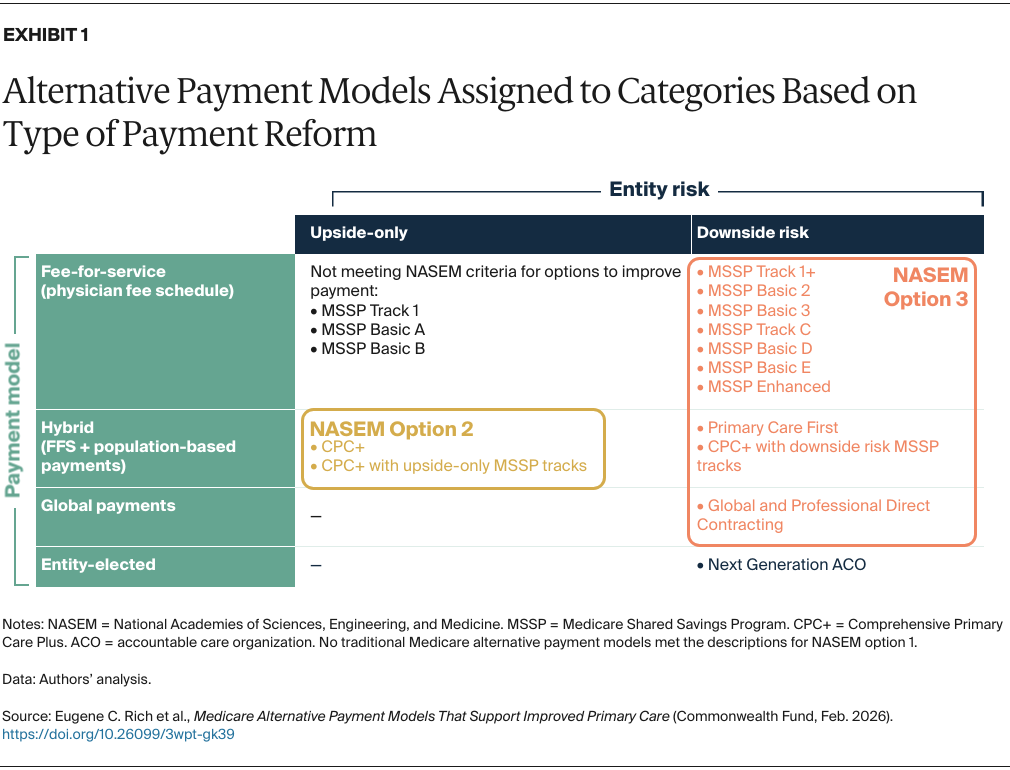
The NASEM framework of options for improving primary care charts three possible paths for reform:
- Option 1: Revisions to the physician fee schedule “to value primary care services more accurately.”
- Option 2: Hybrid payment models which blend fixed, per-patient payments that give providers greater flexibility to deliver the right care at the right time, with fee-for-service for critical preventive services like immunizations.
- Option 3: Broad risk-sharing models where “. . . practices can assume risk accountability in their own contracts, form new entities to participate in risk-sharing models, or participate as part of a larger medical group or integrated delivery system.”
Of the 14 traditional Medicare APMs that CMS put forward, none aligned with the description for enhanced fee schedule payments to primary care (option 1).12 This is not surprising, since increasing fee schedule payments for PCPs would be beyond the statutory scope for developing Medicare APMs unless other requirements were imposed.13
As shown in Exhibit 1, some providers participating in the largest PCP-oriented APM, Comprehensive Primary Care Plus (CPC+), operated under a hybrid payment model (option 2) that blends fee-for-service and fixed, per-patient payments without adding downside financial risk.14 PCPs participating in this model included the subset of CPC+ participants not in a Medicare Shared Savings Program (MSSP) Accountable Care Organization (ACO), as well as those within one of the ACO tracks that did not include downside financial risk to the participating practices.15