Changing how we pay for primary care can incentivize clinicians to deliver the right care at the right time. Historically, clinicians have been retroactively paid a fee for each service they provide. Known as fee-for-service (FFS), this practice encourages clinicians to provide more services, rather than efficiently deliver comprehensive care. Although it can lead to more care, it may not lead to better health outcomes.
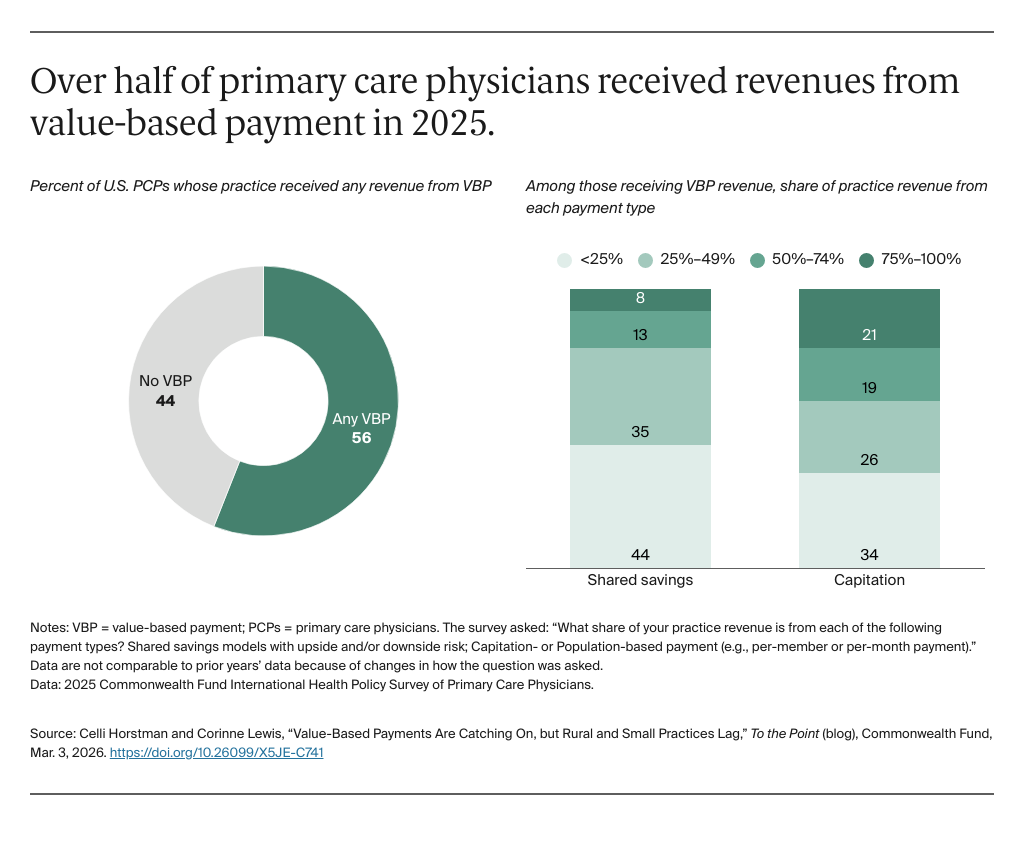
Instead, we could use payment to encourage primary care clinicians to deliver appropriate, efficient care in coordination with other clinicians. An increasingly common way to do this — value-based payment (VBP) — ties clinicians’ payments to their performance on outcomes, including the cost and quality of care. Specific outcomes include the way clinicians manage patients’ chronic conditions or the minimization of avoidable hospitalizations. The evidence shows that changing how we pay for primary can improve patients’ outcomes, including reducing avoidable hospitalizations and increasing access to coordinated care.
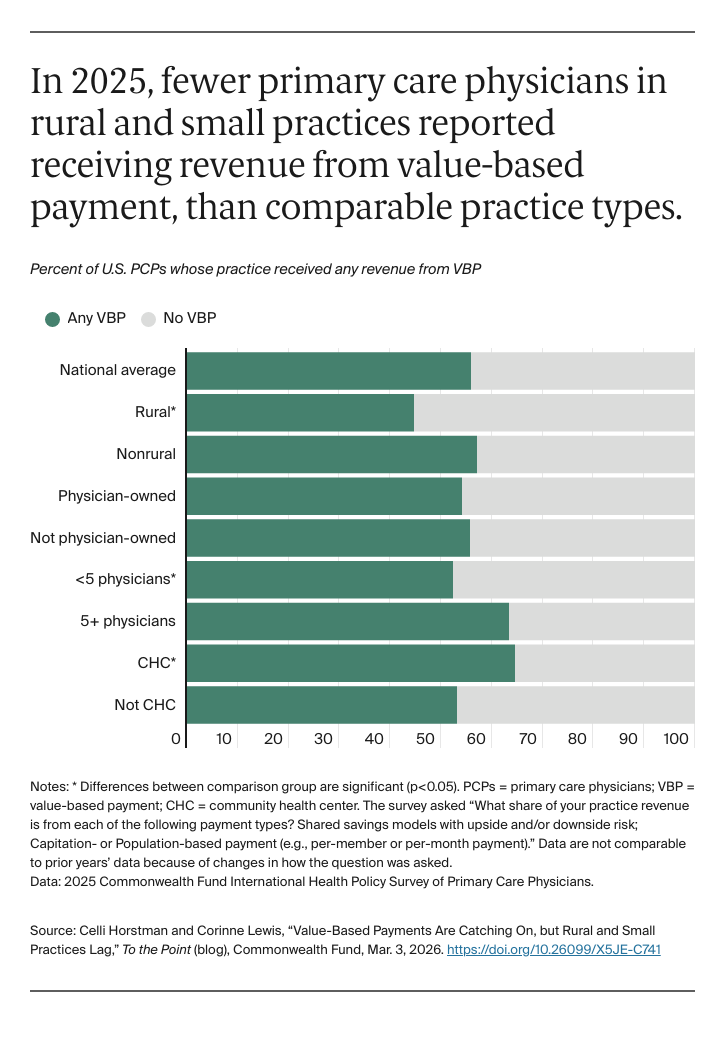
Despite the promise of VBP, some primary care practices have been left behind, and their patients haven’t been able to benefit. Policymakers and payers are particularly worried about low participation among rural, small, and independent practices, as well as community health centers (CHCs) that face unique barriers to participation.
In this blog post, we assess current rates of primary care physician (PCP) participation in VBP, using data from the 2025 Commonwealth Fund International Health Policy Survey of Primary Care Physicians. We also highlight opportunities to design value-based models to account for the needs of different practice settings, such as small or rural practices.