As part of its COVID-19 response, Congress established the $175 billion Provider Relief Fund (PRF) under the CARES Act to compensate for lost revenues providers have experienced as visits have dropped and to help providers respond to the pandemic — for instance, for purchasing personal protective equipment. The law set these two broad uses, leaving it to the U.S. Department of Health and Human Services (HHS) to determine how to distribute funds among providers.
Since April, HHS has allocated funding to different groups of providers in waves and over time and has reclassified payments into two types of distributions. These include general distribution (providers receive at least 2% of annual patient revenue), and targeted distribution (certain providers receive additional payments — for example, payments to hospitals in “hot spots” and to safety-net hospitals). On October 1, HHS announced a new Phase III of the general distribution, indicating that payments will take account of providers’ revenue losses and expenses attributable to COVID-19 and the PRF payments they have received to date. However, HHS did not provide the payment methodology.
To date, community-based providers (i.e., noninstitutional providers, such as behavioral health clinics and pediatricians) that serve Medicaid and uninsured patients have been disadvantaged by this distribution model in three ways:
- they are disadvantaged by the rules for calculating general distribution payments
- with the exception of rural health centers, they have been left out of the targeted distributions
- the PRF is administratively complex and challenging for tightly staffed, small practices to navigate.
Without more support, these providers are at risk of closing, which will lead to ongoing challenges in health care access in the very communities most impacted by COVID-19.
General Distribution Methodology to Date Disadvantages Medicaid Providers
The basic premise of the general distribution is that all providers will receive at least 2 percent of net patient revenue. Under the new Phase III distribution, some providers (though it is unclear exactly which ones) will receive additional payments.
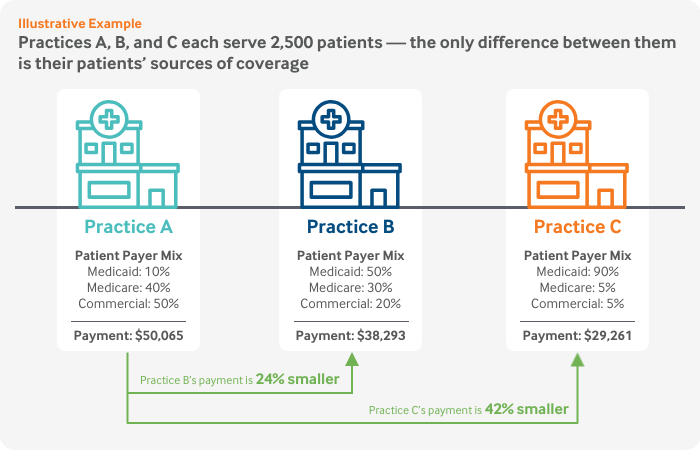
Basing payments on patient revenue means the highest per-patient payments go to providers with a large proportion of privately insured patients and the lowest go to providers with a high percentage of Medicaid patients. In other words, the least-well-resourced providers with the lowest patient revenue and thinnest margins receive the smallest general distribution payments.
This figure illustrates how the methodology plays out for three hypothetical practices that are identical in every way, except for their patients’ sources of coverage.